• ANEMIA
• Definition
•Anemia is a condition where the hemoglobin content of the blood is
below the normal level for the age and sex of the subject.
• Anemia means deficiency of hemoglobin in the blood, which can be caused by
too few RBCs or too little hemoglobin in the cells (GYTON)
.
• Signs andSymptoms of Anemia
• . Pallor of skin & mucous membrane is most evident sign of
anemia.
• . Anemia reduces oxygen carrying capacity of blood, resulting in
tissue hypoxia.
• . Decrease in viscosity of blood and increase in cardiac output
produces turbulence of blood during its passage through heart
producing cardiac murmurs.
• . Dry skin, brittle nails, glossitis, atrophy of papillae of tongue,
restlessness, etc., are other features.
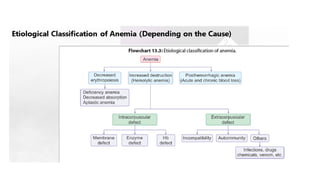
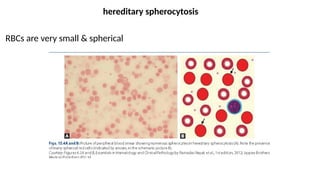
• I. Hemolyticanemia (due to increased destruction of RBC)
• . Intracorpuscular defects:
Abnormality in RBC membrane as in hereditary spherocytosis
Disorders of glycolysis due to enzyme defect like G6PD deficiency
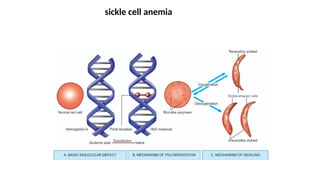
Abnormality in globin structure of hemoglobin as in thalassemia, sickle cell anemia, etc.
• . Extracorpuscular defects:
Incompatible blood transfusion
Infections like malaria
Autoimmune hemolytic anemia
Drugs
Snake venom
10.
• II. Anemiadue to defective formation of RBC
• . Deficiency of essential substances like iron, folic acid, vitamin
B12, protein, Co, Cu, , etc.
• . Defective absorption of essential substances.
• For example, intrinsic factor deficiency leads to pernicious
anemia; HCl and vitamin C deficiency leads to iron deficiency
anemia.
• . Atrophy of bone marrow leads to aplastic anemia.
• Causes are drugs like sulfa group, ionizing radiation in treatment
for cancer, malignancy of bone marrow as multiple myeloma, etc.
11.
• III. Post-hemorrhagicanemia
• . Acute blood loss following accident, childbirth, etc.
• . Chronic blood loss as in hookworm infestation, which most
common cause of anemia in children, bleeding piles, bleeding
peptic ulcer, etc.
Hypochromic Microcytic Anemia
•MCV, MCH, & MCHC are below normal.
• Micronormoblasts are seen in bone marrow
• result of a defect in red cell formation in which hemoglobin synthesis is
impaired.
.I Iron-deficiency anemia
ii. Thalassemia
14.
Normochromic Normocytic Anemia
•MCV, MCH, & MCHC are within the normal range.
• i. blood loss anemia
• ii. hemolytic anemia
• iii. bone marrow failure or chronic renal failure (aplastic anemia).
15.
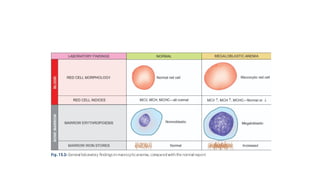
Macrocytic Normochromic Anemia
•The MCV is above the upper limit of the normal.
• Megaloblasts are seen in bone marrow examination . Howell Jolly body,
hypersegmentation of neutrophils, basophilic stippling are also seen
• megaloblastic anemia -deficiency of vitamin B12 or folic acid
16.
Common Anemias
Iron-deficiency Anemia(IDA)
• Commonest form of anemia in developing countries.
• three major factors
• 1. Increased physiological demand for iron as occurs in pregnancy, lactation, growing children.
• 2. Inadequate iron intake
• 3. Pathological blood loss like bleeding peptic ulcer,piles, worm infestations, epistaxis, hemoptysis etc.
• microcytic hypochromic type.
• micronormoblasts in bone marrow
• decreased MCV, MCH & MCHC
• dcreased marrow iron store
18.
Blood Loss Anemia
Afterrapid hemorrhage, body replaces fluid portion of plasma in 1 to 3 days, but
this response results in a low concentration of RBCs.
If a second hemorrhage does not occur, RBC concentration usually returns to
normal within 3 to 6 weeks.
When chronic blood loss occurs, a person frequently cannot absorb enough iron
from intestines to form hemoglobin as rapidly as it is lost. RBCs that are much
smaller than normal and have too little hemoglobin (microcytic hypochromic
anemia)
19.
Aplastic Anemia Dueto Bone Marrow Dysfunction.
• high-dose radiation or chemotherapy for cancer treatment can damage stem cells
• of bone marrow, followed in a few weeks by anemia.
• high doses of certain toxic chemicals, such as insecticides or benzene in gasoline
• In autoimmune disorders, such as lupus erythematosus, immune system begins
attacking healthy cells such as bone marrow stem cells,
• half of aplastic anemia cases the cause is unknown, a condition called idiopathic
aplastic anemia.
• People with severe aplastic anemia usually die unlessthey are treated with blood
transfusionsor by bone marrow transplantation.
20.
Megaloblastic Anemia.
vitamin B12, folic acid, & intrinsic factor loss lead to slow reproduction of
erythroblasts in bone marrow.
• As a result, the RBCs grow too large, with odd shapes, and are called
megaloblasts.
• DNA synthesis & RBC maturation are decreased
22.
• Pernicious Anemia
•lack of intrinsic factor of Castle leading to defective
absorption of vitamin B12 in distal ileum.
Thalassemia
• Thalassemia isa genetically determined heterogenous group of commonest
monogenic disorder in which rate of synthesis of one or more types of
hemoglobin polypeptide chain is decreased.
• Thus, there are two major classes of thalassemia: α thalassemia and β
thalassemia,
• In β thalassemia (failure to synthesize β chain), which is more common, there is
excess α chain production that damages red cell precursor and red cells.
• 1. There are major and minor forms of the disease.
• 2. In β thalassemia major, anemia develops in first few months of life and
becomes progressively severe.
27.
EFFECTS OF ANEMIAON CIRCULATORY SYSTEM FUNCTION
• blood viscosity may fall to as low as 1.5 times that of water rather than normal
value of about 3.
• In turn decreases resistance to blood flow in peripheral blood vessels
• Then greater than normal quantities of blood flow through tissues & return to
heart,
• thereby greatly increasing cardiac output.
• And increased pumping workload on heart
28.
POLYCYTHEMIA
• Secondary Polycythemia.
•Whenever tissues become hypoxic because of too little oxygen in breathed air,
such as at high altitudes (physiological polycythemia )or because of failure of
oxygen delivery to tissues, such as in cardiac failure, ------produce large
quantities of extra RBCs.
• RBC count commonly rises to 6 to 7 million/mm3,
29.
Polycythemia Vera (Erythremia)(primary form)
• pathological condition RBC count may be 7 to 8 million/mm3
• hematocrit may be 60% to 70% .
• genetic aberration in hemocytoblastic cells ,blast cells no longer stop producing RBCs
• excess production of white blood cells & platelets as well.
• total blood volume also increases,
• viscosity of the blood increases from normal of 3 times viscosity of water
to 10 times that of water.
30.
Relative or apparentpolycythemia
is not true polycythemia,
increase in red cells due to dehydration
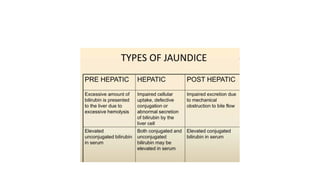
• Jaundice, alsoknown as icterus, is the yellowish discoloration of the
skin, whites of the eyes (sclera), and mucous membranes. This
happens due to an excess accumulation of bilirubin in the blood, a
condition called hyperbilirubinemia.
• Jaundice. The plasma bilirubin concentration normally does not
exceed 17 μmol/L (= 1 mg/dL). Concentrations higher than 30 μmol/L
(1.8 mg/dL) lead to yellowish discoloration of the sclera and skin,
resulting in jaundice (icterus)
36.
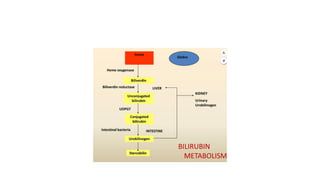
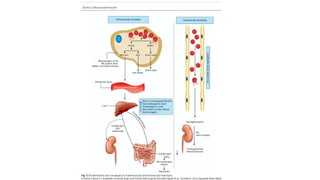
• Enterohepatic circulation
•substances like bile acids, bilirubin, & certain drugs are transported from
liver to small intestine, then reabsorbed & sent back to liver.
• This "recycling" system allows body to efficiently reuse bile salts for
digestion & maintains a constant bile acid pool in healthy individuals.
• However, it significantly extend half-life of certain medications by allowing
them to be reabsorbed after being excreted