Downloaded 380 times
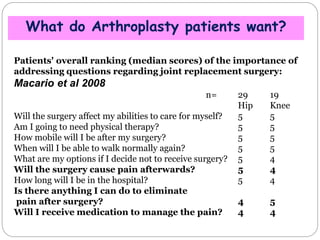
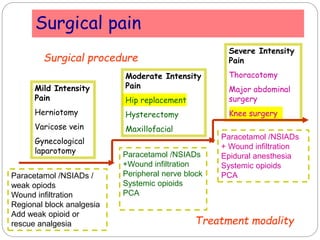
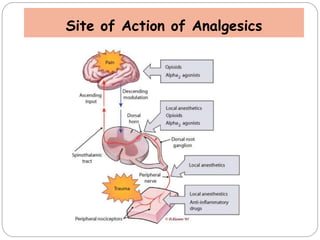
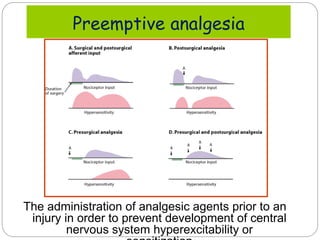


The document discusses key concepts in pain management following hip and knee arthroplasty. It defines pain and discusses what patients want after surgery like mobility and pain management. It outlines the benefits of a multimodal approach using techniques like neuraxial blocks, peripheral nerve blocks, and local infiltration to provide good pain relief with fewer side effects than opioids alone. This multimodal, balanced approach can lead to early mobilization, recovery and discharge from the hospital.










































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)


















