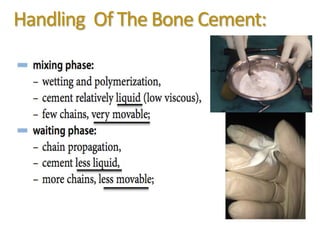
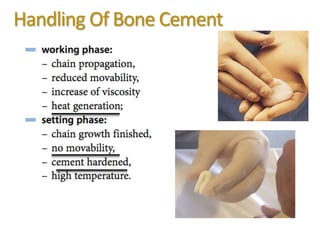
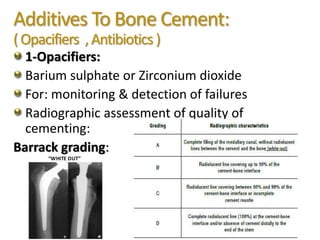
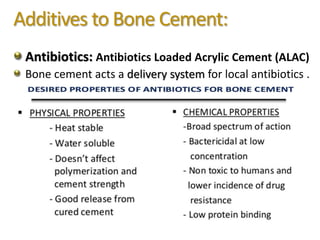
This document discusses bone cement, providing its history, composition, polymerization process, and techniques for use. Bone cement is composed of PMMA powder and methyl methacrylate liquid that undergo radical polymerization to form polymers. Proper bone cementing techniques like pulsatile lavage, vacuum mixing, and pressurization improve cement quality and fixation. Additives like antibiotics and opacifiers are used but can affect cement properties. Occupational and patient hazards like cement implantation syndrome require prevention through management of vapor exposure and embolic risks.