Downloaded 769 times


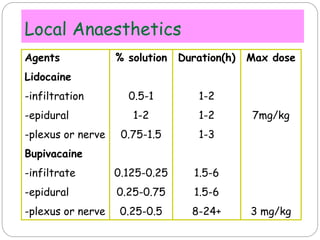
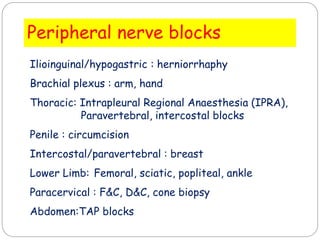



This document discusses key concepts in post-operative pain management. It defines types of pain and outlines consequences of poorly managed acute post-operative pain such as increased risk of chronic pain, medical complications, and decreased patient satisfaction. The document reviews various analgesic agents including acetaminophen, NSAIDs, opioids, local anesthetics, and the benefits of a multimodal approach. Regional anesthesia techniques like peripheral nerve blocks and epidural analgesia are presented as effective options for post-operative pain control.





























































































