Downloaded 222 times






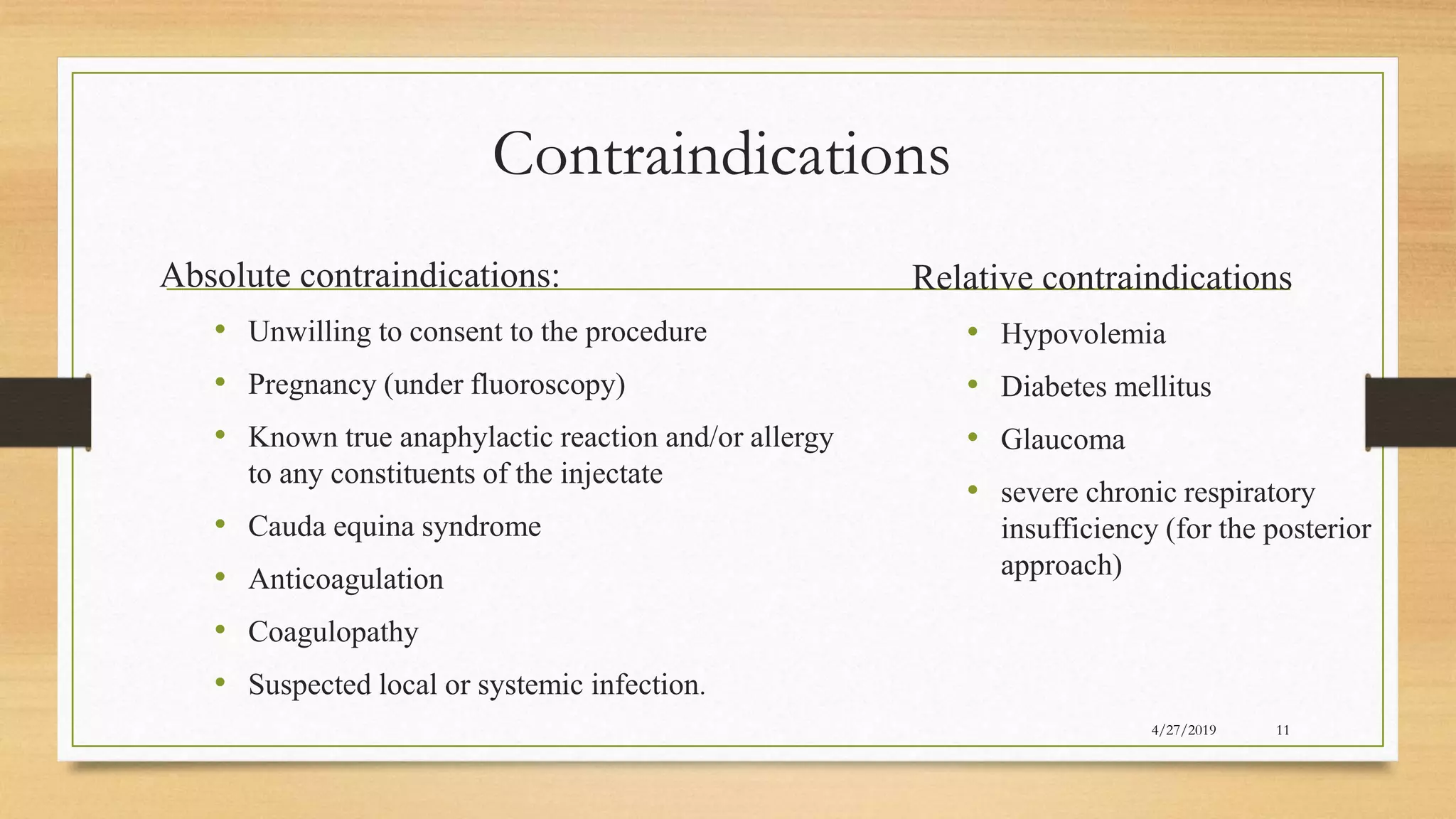


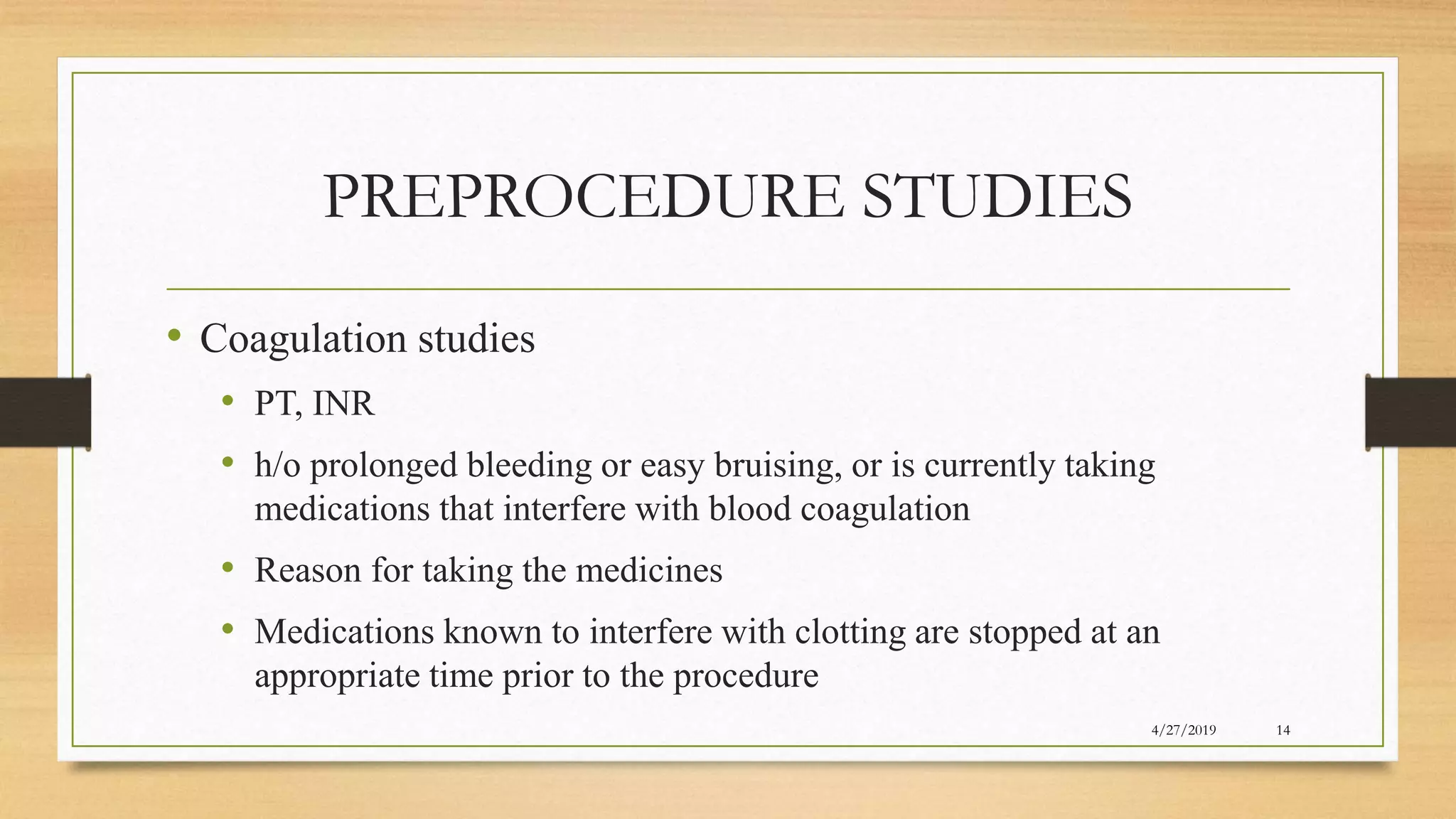























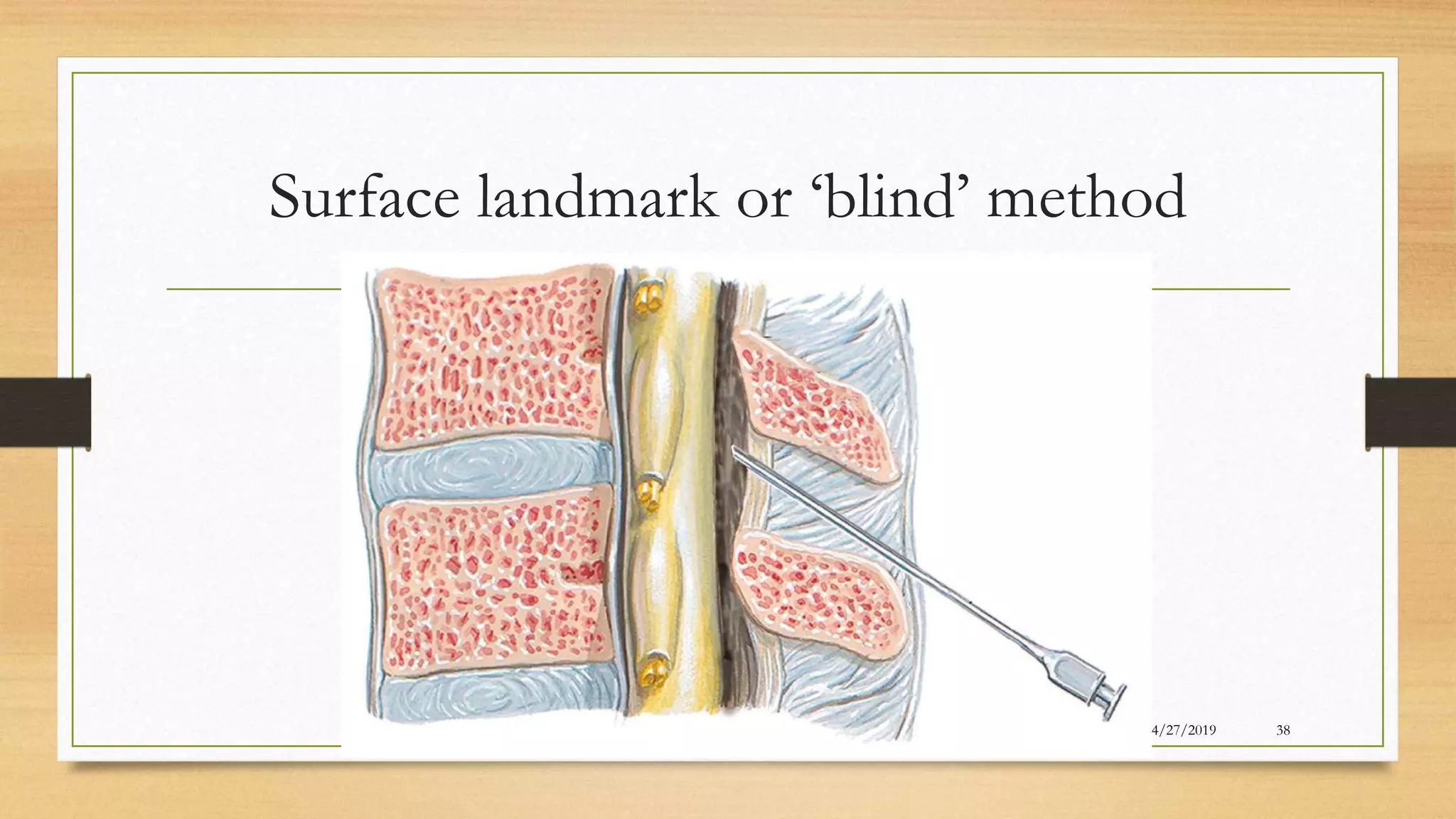





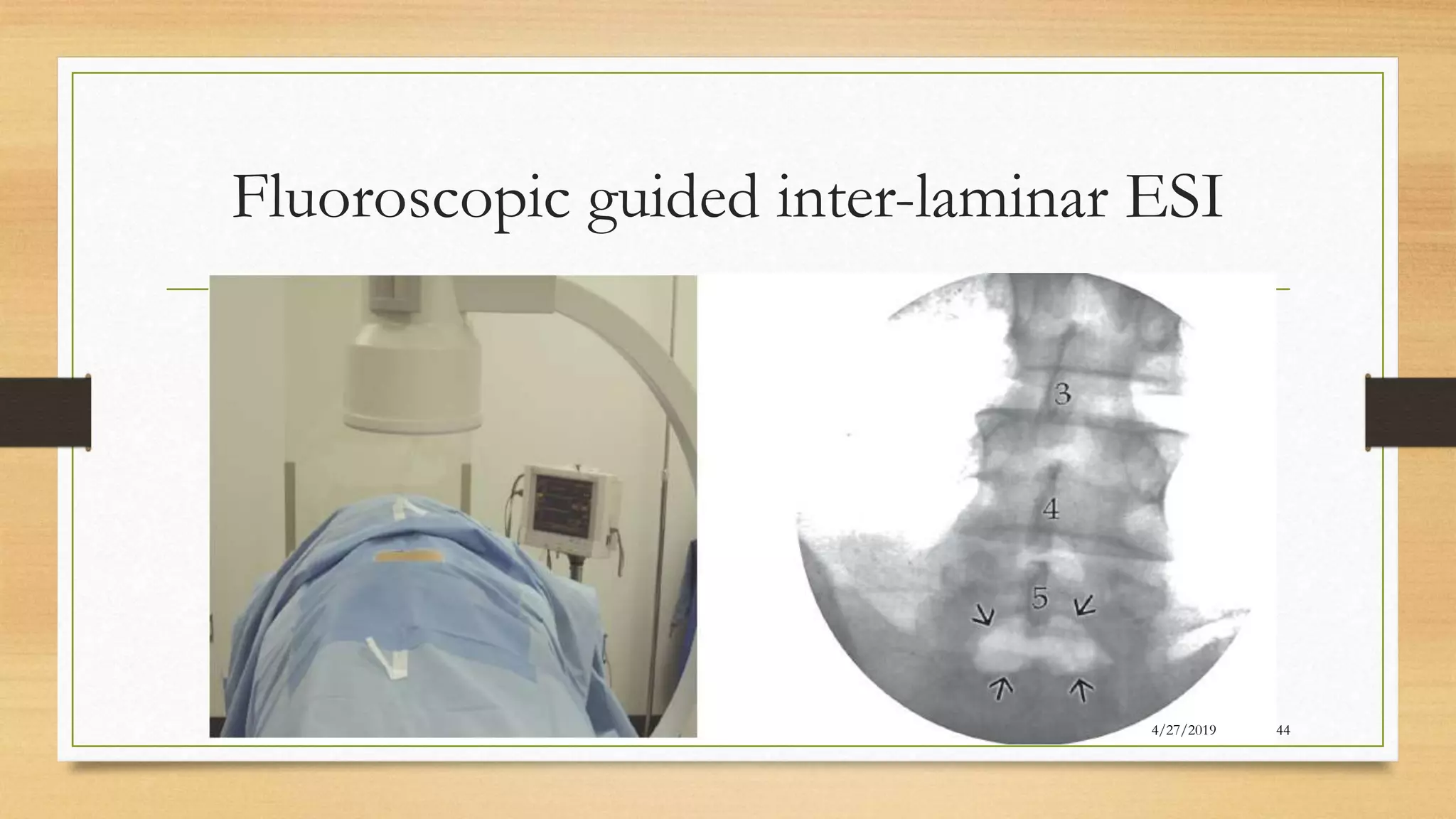
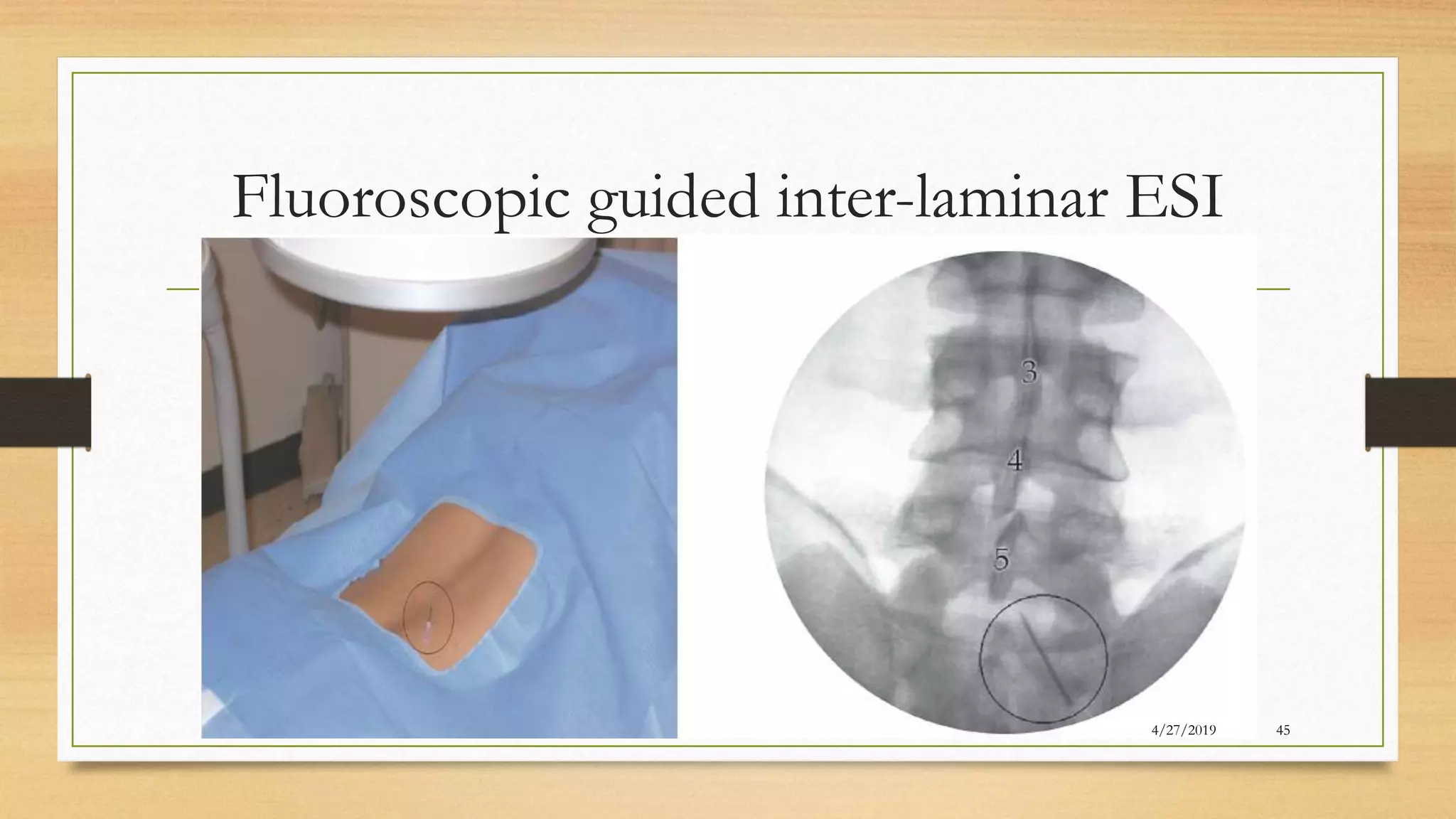

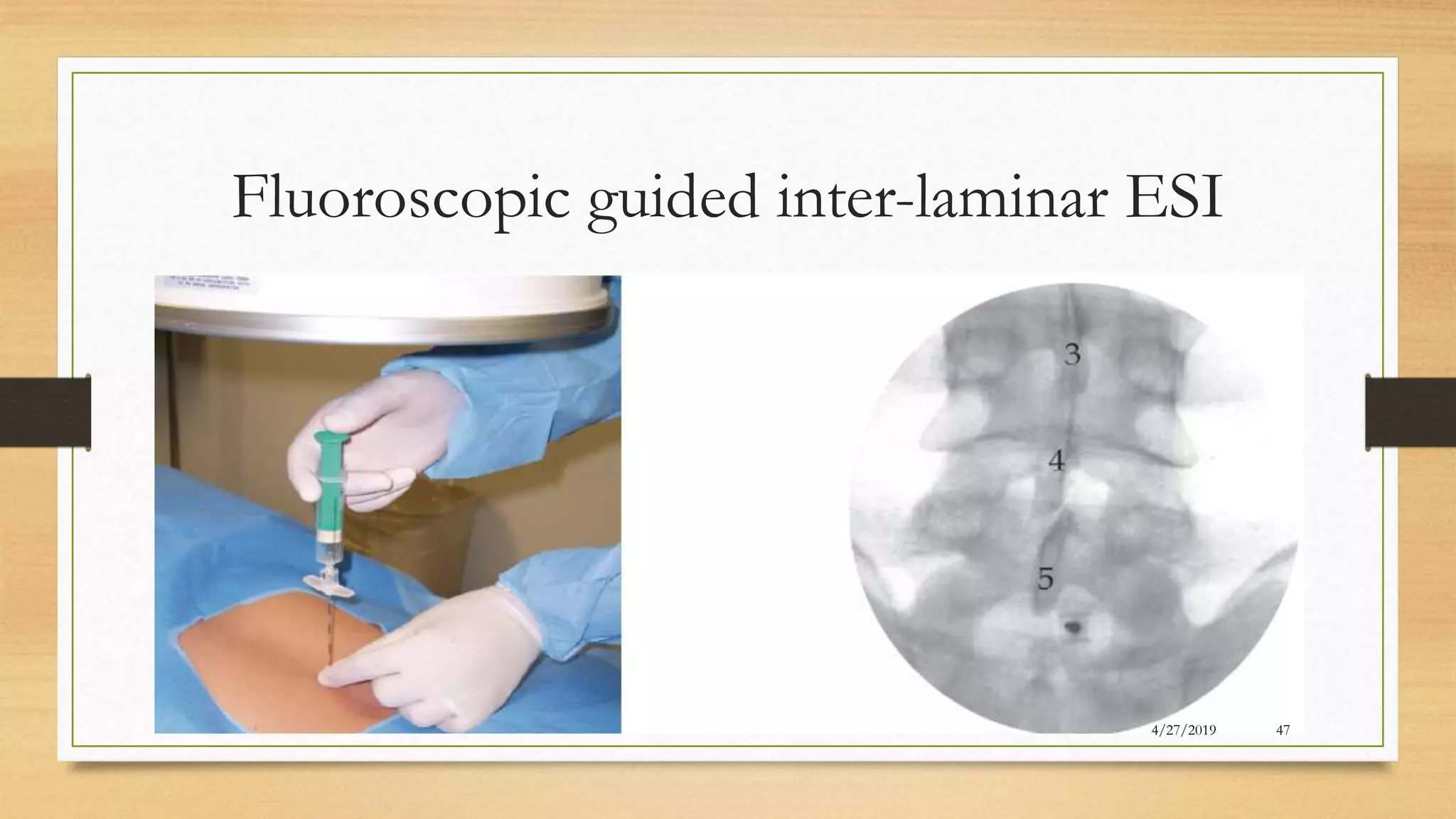






































The document discusses the use of epidural steroid injections (ESI) for treating low back pain and associated conditions, highlighting their prevalence, indications, contraindications, and mechanisms of action. It emphasizes the importance of fluoroscopic guidance for accurate needle placement and outlines both the short-term and moderate long-term efficacy of ESIs for conditions like radiculopathy and spinal stenosis. Additionally, it addresses potential complications related to both the procedure and steroid administration.










































































