This document summarizes a presentation on anaesthesia and pain relief given by Dr. Annush Tha. It covers various topics including:
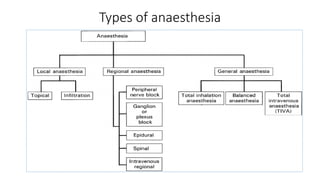
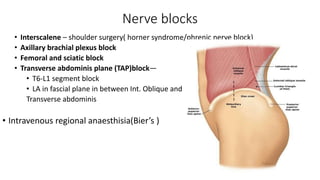
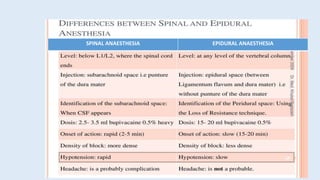
- Types of anaesthesia such as general, local, and regional anaesthesia along with their techniques and monitoring.
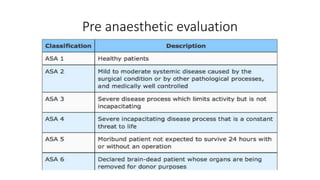
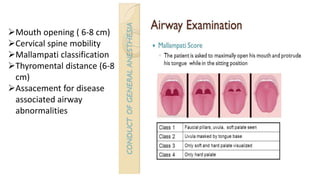
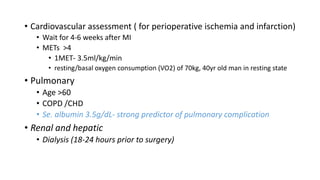
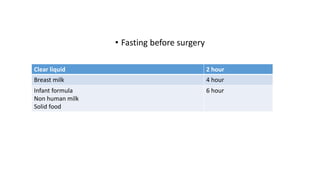
- Pre-anaesthetic evaluation and selection of anaesthetic technique based on factors like operative site and patient risk.
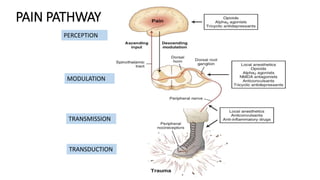
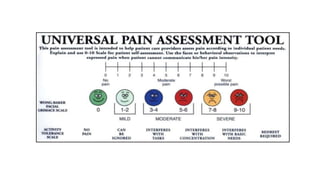
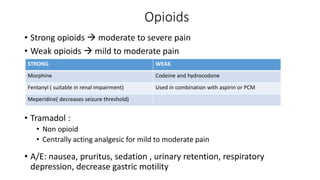
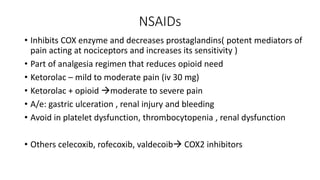
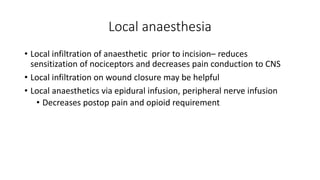
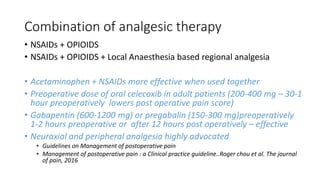
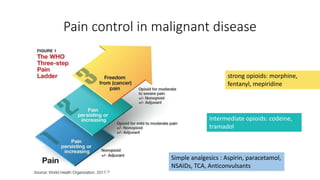
- Acute and chronic pain management with a focus on multimodal approaches using analgesics like opioids, NSAIDs, and local anaesthetics.
- Special considerations for pain control in malignant diseases and chronic pain conditions.
The key messages are that anaesthesia selection should be tailored per patient and surgery with cost in mind, multimodal pain

















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











