Download as PDF, PPTX











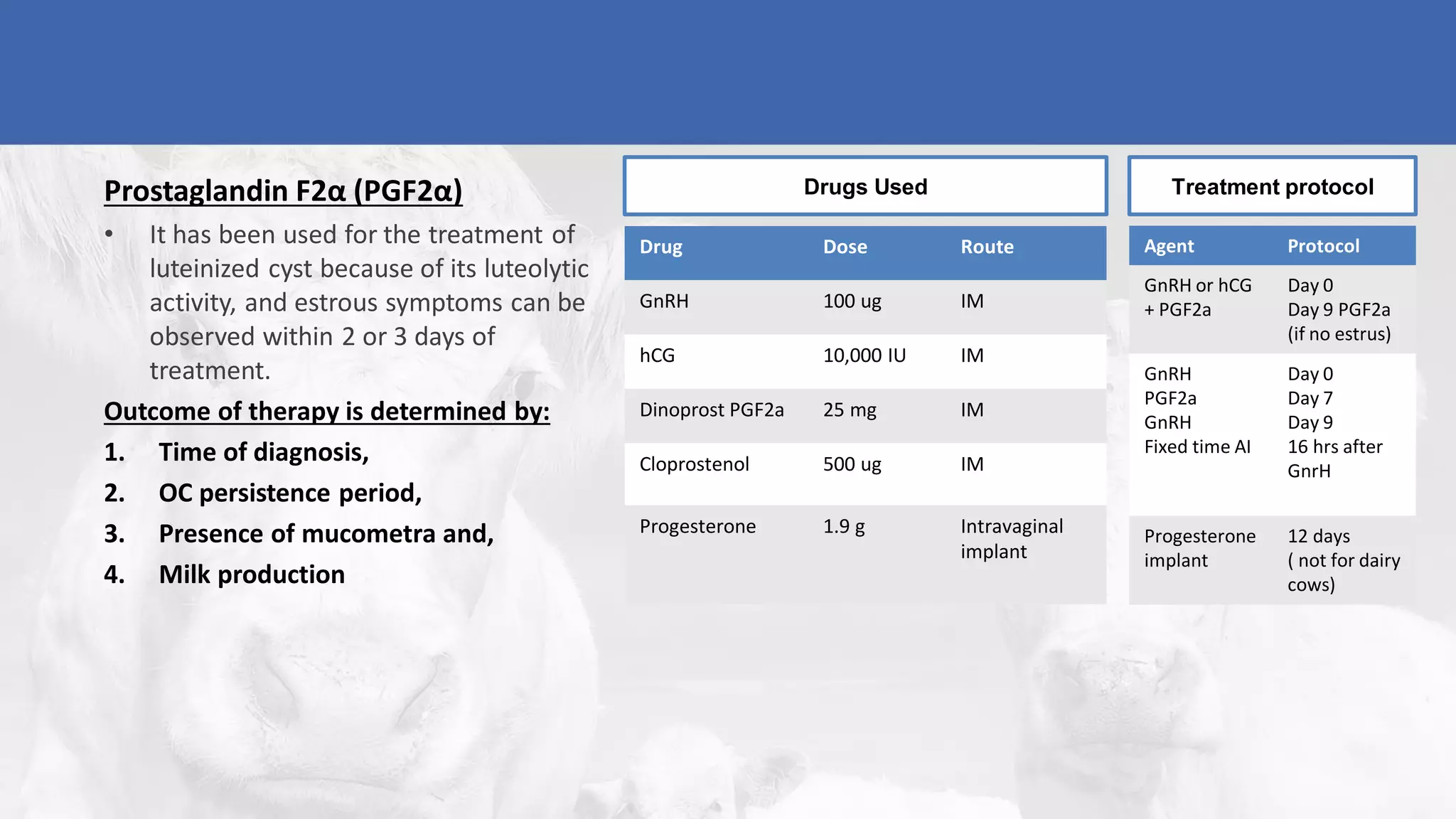


1) Cystic ovarian degeneration is a condition in dairy cows where ovarian follicles fail to ovulate, continuing to grow into cysts. It commonly occurs 30-60 days after calving and can impair fertility. 2) Ovarian cysts are diagnosed using history, palpation, ultrasound to detect enlarged follicles over 17mm in the absence of a corpus luteum, and progesterone assays. 3) Common treatments include a single injection of GnRH or hCG to induce luteinization and ovulation, followed by a prostaglandin injection 9 days later if needed to induce estrus. This summary effectively captures the key details about cystic ovarian degeneration in cattle.



































































