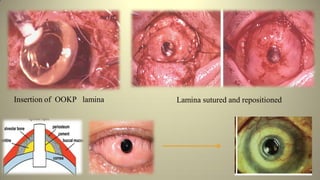
This document discusses the osteo-odonto-keratoprosthesis (OOKP), a surgical procedure used to treat corneal blindness. It involves implanting an artificial cornea attached to a patient's tooth and bone. The OOKP provides the best option for restoring vision in severe corneal disease. The procedure is complex, involving both ophthalmological and oral surgeons. It has high success rates but also risks like infection. Lifelong follow up is required as it is a two-stage surgery. Overall, the OOKP offers a successful method of visual rehabilitation for corneal blindness.