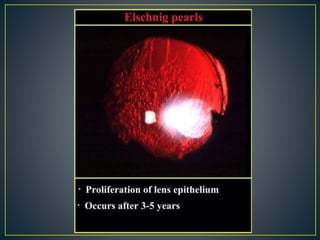
Visually significant posterior capsular opacification (PCO), also known as after cataract, is the most common complication of cataract surgery, occurring in 20-25% of patients. It is caused by the proliferation of lens epithelial cells remaining in the capsular bag after surgery. Symptoms include blurry vision, glare, and sometimes double vision. Treatment involves using a Nd:YAG laser to create an opening in the posterior capsule. This procedure is called a posterior capsulotomy and effectively treats PCO symptoms.