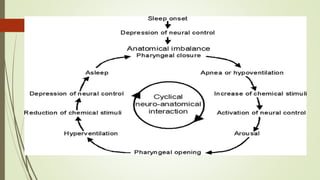
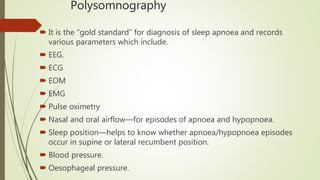
Snoring and obstructive sleep apnea occur when the muscles in the back of the throat relax during sleep, causing vibration that produces snoring sounds or complete or partial airway obstruction. Obstructive sleep apnea is defined by cessation of breathing lasting 10 seconds or more during sleep and is classified based on the respiratory disturbance index. Polysomnography is the gold standard test used to diagnose sleep apnea and involves monitoring various physiological parameters during sleep. Treatment options include lifestyle changes, oral appliances, continuous positive airway pressure therapy, and various surgical procedures to reduce tissue volumes or advance structures in the throat.










































![OBSTRUCTIVE SLEEP APNEA [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/obstructivesleepapneaautosaved-240801041633-6b724373-thumbnail.jpg?width=640&height=640&fit=bounds)













































