Downloaded 111 times













![- In OPG, when mesiodistal width of canine crown was 1.5 times larger
(i.e. 15% larger) than the adjacent central incisor, then the canine is
palatally placed.
- This is only true in cases where canine should not be at a higher level.
[Reliability of a method for localisation of displaced maxillary canines using a
single panoramic radiograph. Chaushu et al; clin orthod res 1999; 2: 194-9]](https://image.slidesharecdn.com/managementofimpactedcanines-210503081220/75/Management-of-impacted-canines-31-2048.jpg)

























































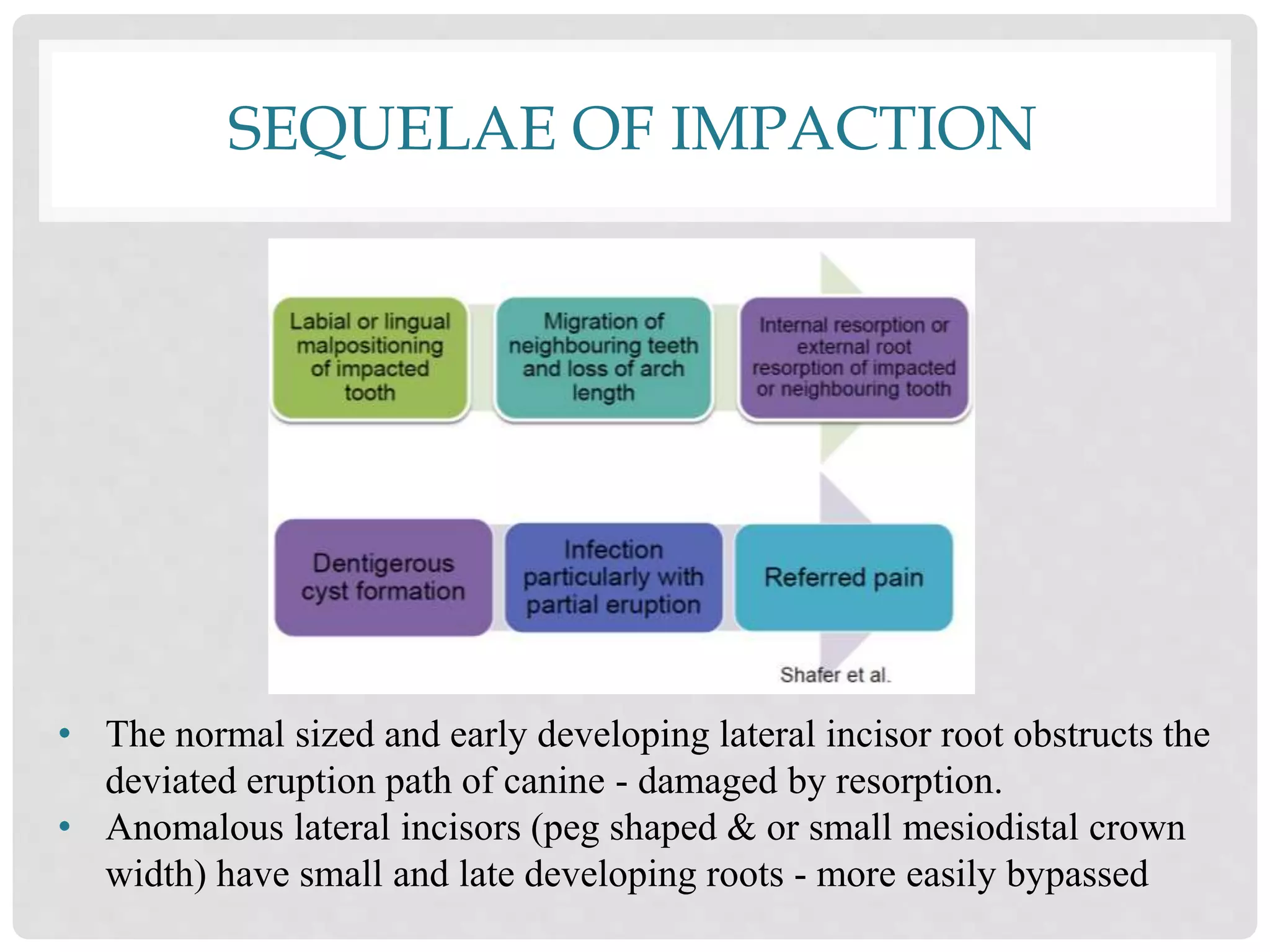
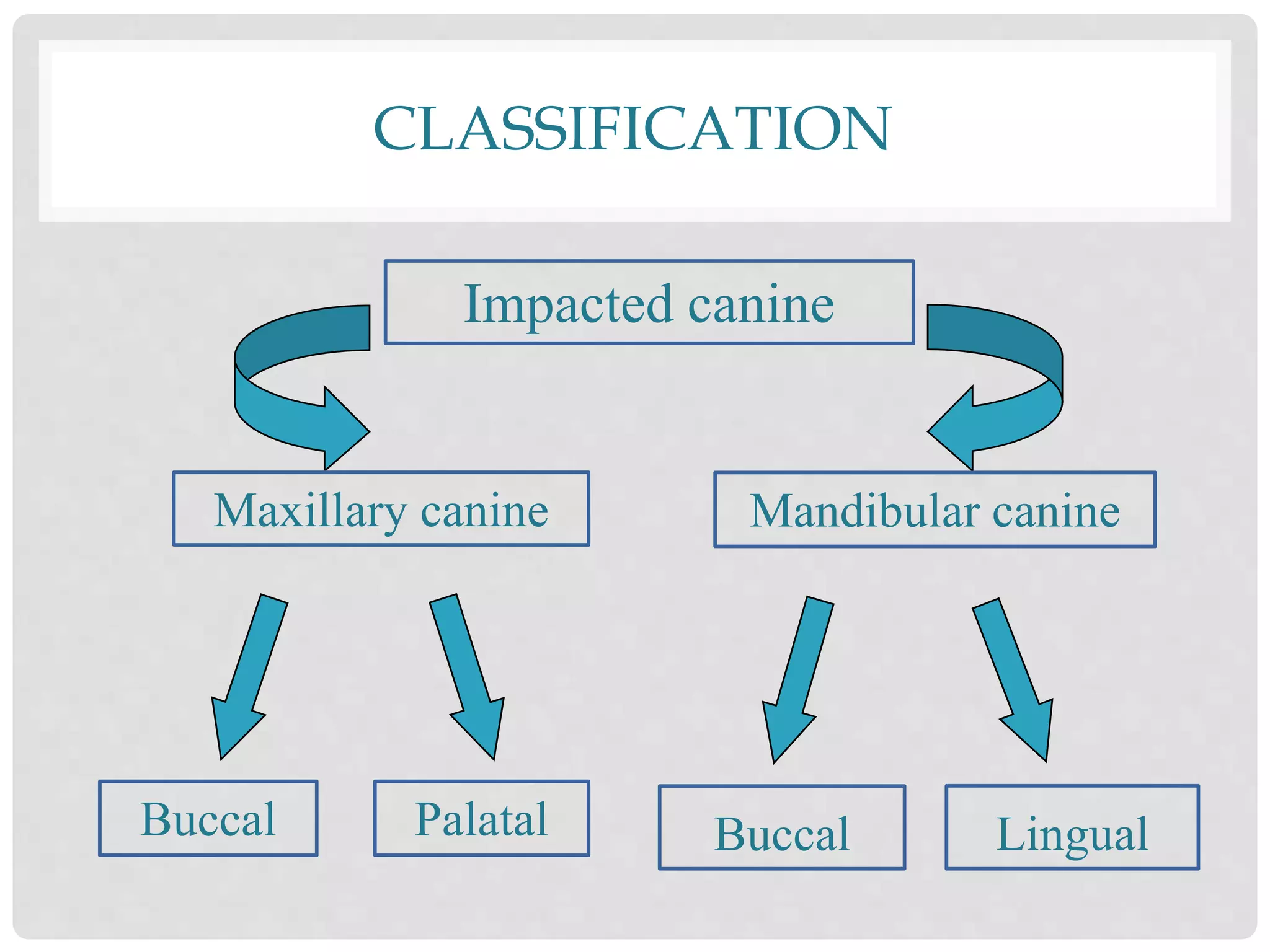
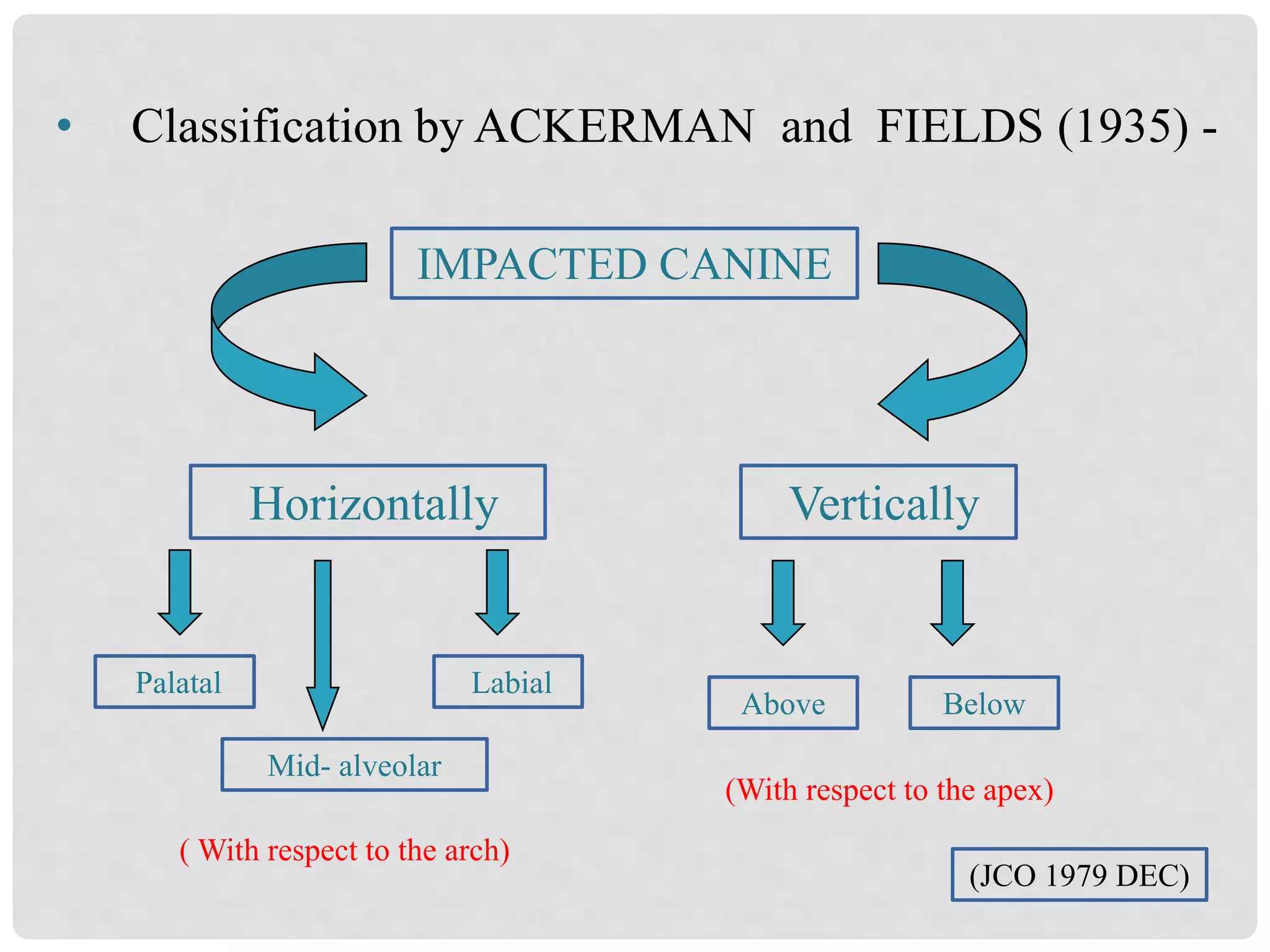
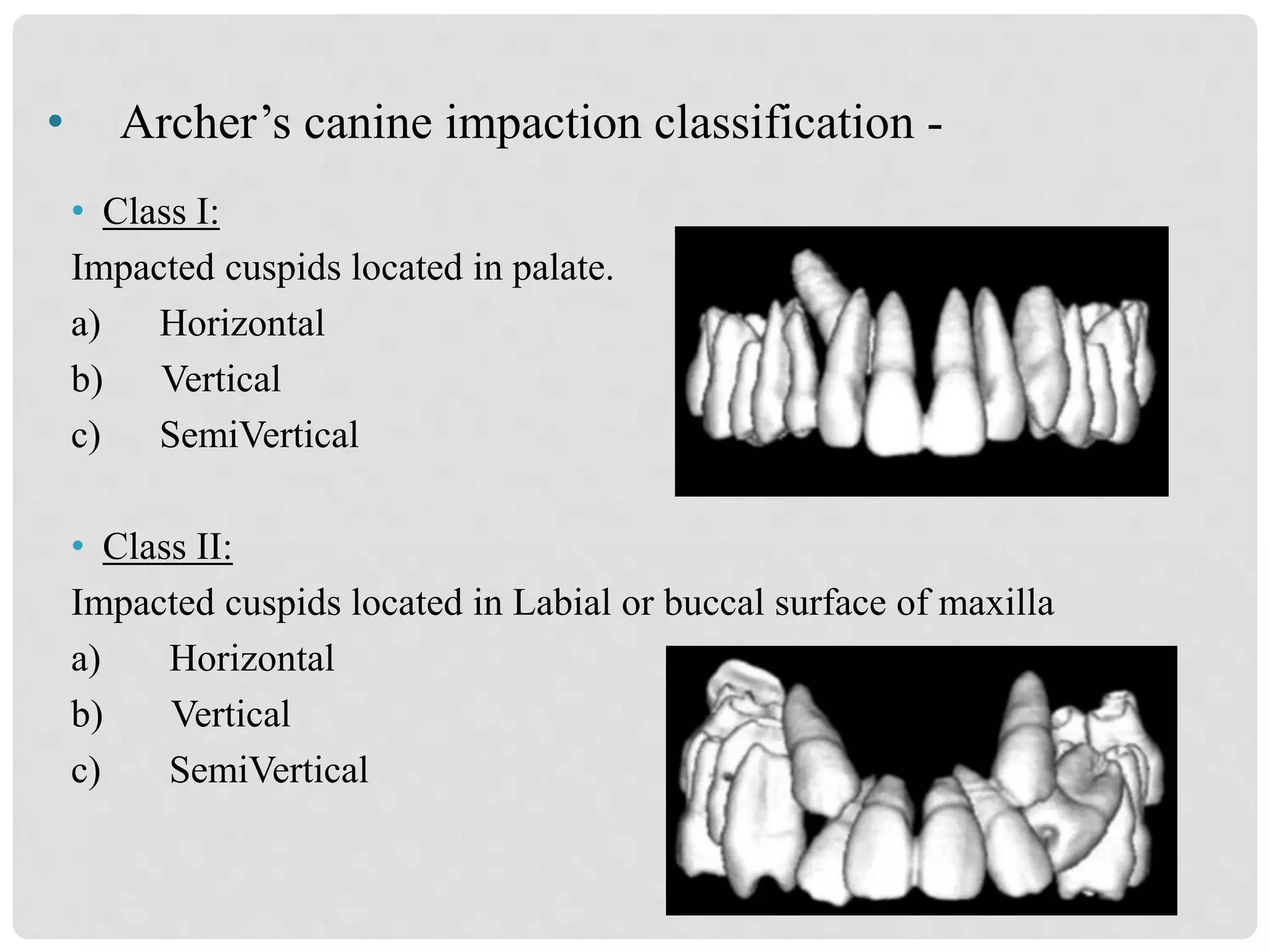
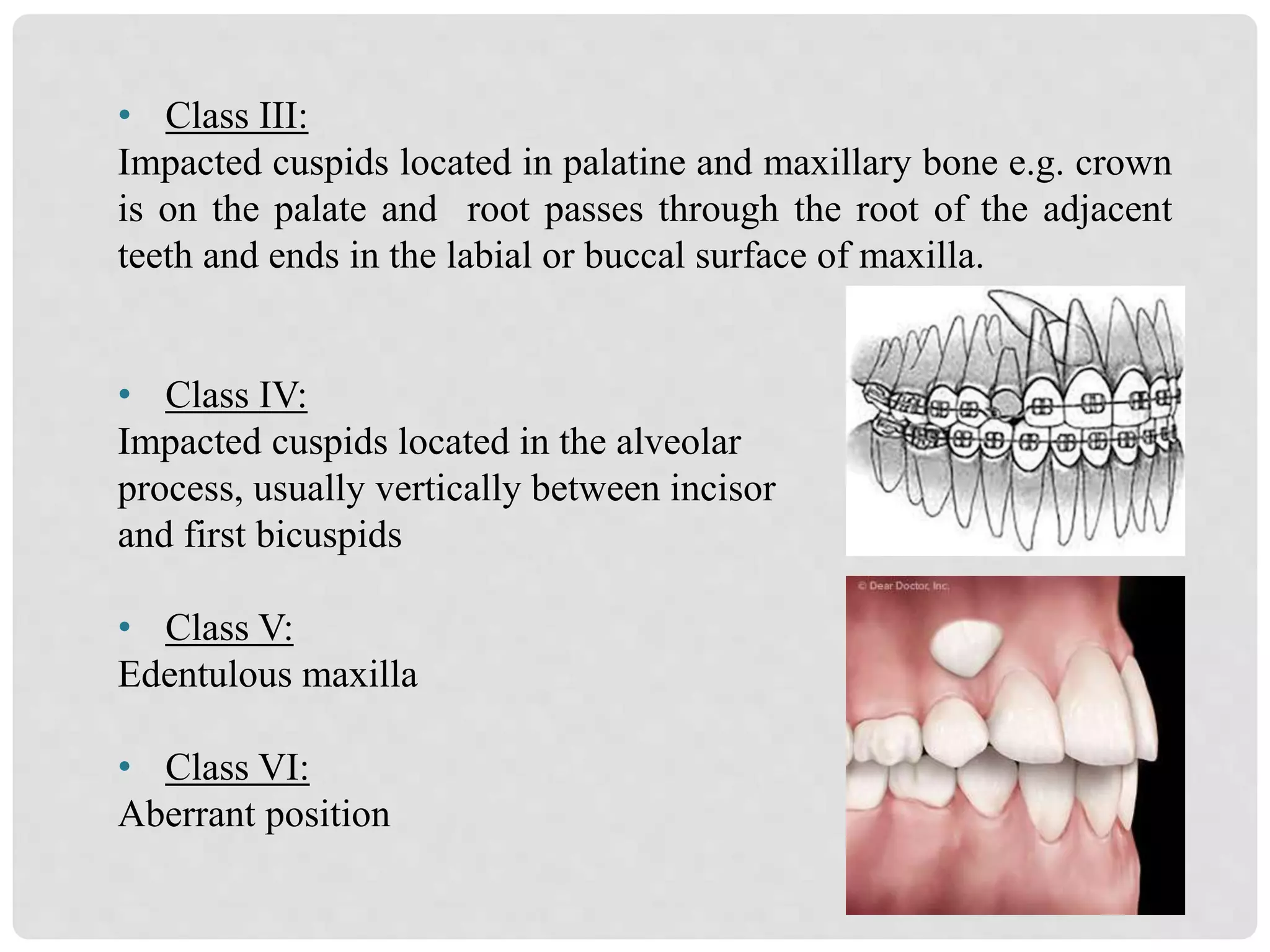
The document outlines the management of impacted canines, discussing their incidence, development, etiology, diagnosis, and treatment options. It highlights the common occurrence of maxillary canine impaction, particularly in females, and categorizes various classifications and complications associated with impacted canines. Additionally, it emphasizes the importance of clinical and radiographic evaluations in diagnosing and predicting the prognosis of impacted canines.
















![FACEMASK CHINCUP SEMINAR[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/facemaskchincupseminar1-230916061625-e0964de8-thumbnail.jpg?width=640&height=640&fit=bounds)































































