3. Con….
Cyclospora was first reported in Papua New
Guinea in 1979 as an oocystlike body found in
3 patients with intestinal infections.
Disease caused by Cyclospora is known as
Cyclosporiasis.
Infection is self–limiting in immunicompetent
host.
5. Geographical distribution
Tropical & sub tropical countries.
Cyclosporiasis is endemic in Nepal,Peru
&Haiti.
INDIA: Sporadic cases of infections are
reported from Vellore ,Pondicherry,New Delhi
& Banglore.
6. Cyclospora Infection among School Children in Kathmandu, Nepal: Prevalence
and Associated Risk Factors
Published online 2015 Aug 20. doi: 10.2149/tmh.2015-25
The intestinal coccidian protozoa Cyclospora cayetanensis has emerged as an
important cause of parasitic diarrhea among children living in developing
countries. This study aimed to determine the prevalence
of Cyclospora among the school children of Kathmandu with reference to
various associated risk factors.
A total of five hundred and seven stool samples from students between the
age of 3–14 years, studying in 13 different schools in Kathmandu were
collected during the study period (May–November, 2014) and processed at
the Public Health Research Laboratory, Institute of Medicine, Kathmandu,
Nepal. A modified acid fast staining technique (Kinyoun’s method) was used
to detect oocyst of Cyclospora from the formal-ether concentrated stool
samples.
Cyclospora was detected in 3.94% (20/507) of the stool samples examined.
The prevalence was found to be highest among the students in the 3–5 year
age group i.e. 10.15% (13/128), peaking during the rainy season (June–
August).
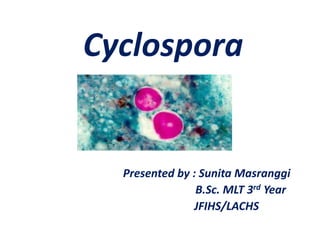
7. Morphology
Oocysts are spherical, non –
refractile,8-10 micro meter in
diameter.
Contains two sporocysts,each
sporocyst contains two
sporozoites.
Readily detected with
conventional microscopy.
On modified acid-fast smears,
the oocyst will stain from a
light pink to a deep red.
11. Life cycle
Typical of all enteric coccidial
infections
Ingestion of a sporulated oocytes ( each
containing 2sporocytes with 2sporozoites
enclosed within)
Sporozoites penetrate epithelial cells of small
intestine (especially jejunum)
12.
13. Merogony
Undergo multiple fission to
form meronts, which contain
multiple merozoites (2 generation)
– type I meronts (8-12 merozoites)
– type II meronts (4 merozoites)
Later generation merozoites
penetrate new cells and forms
Gametes.
14. Gamogony
Most gametes enlarge,
forming the female
macrogamete.
A few become sperm-like
microgametes which fertilize
the macrogametes.
Oocyst wall is layed down around zygote.
Unsporulated oocyst sloughs from intestinal wall
and is passed in the feces.
15. Sporogony ( sporulation)
Development of sporocysts
and sporozoites.
Occurs only in the presence
of higher atmospheric oxygen
concentration, particularly in
warm, wet soil.
Complete within 7-12 days.
20. Host Factors that influence
disease
People of all ages.
Young children &
immunocompromised individuals.
21. Signs and symptoms
Apper 1week after ingestion of oocyst
Prolonged watery diarrhea
weight loss
Anorexia
myalgia
Occasionally vomiting and fever
Mild infection with few or no clinical signs may
occur
22. Laboratory diagnosis
Microscopic Examination of
stool sample.
Lacto Phenol Cotton Blue(LPCB):
wet mount of stool smear.
Concentration Method
Formalin Ether sedimentation technique
24. Autofluorescent, meaning
that when stool containing
the parasite is viewed under
an ultraviolet (UV) fluorescence
the oocysts appear
blue or green against a black
background.
Molecular technique: PCR