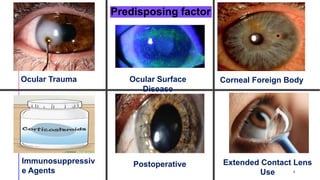
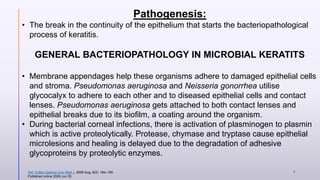
This document provides information on bacterial keratitis including its definition, demographic data, predisposing factors, pathogenesis, symptoms, clinical presentation, diagnostic testing, and treatment. Bacterial keratitis is an infection of the cornea associated with a corneal infiltrate and epithelial defect caused by bacteria. It most commonly affects contact lens users and individuals with ocular trauma or surface disease. Clinical presentation depends on the causative organism, with Gram-positive cocci like staphylococci causing well-defined lesions and Gram-negatives like Pseudomonas typically progressing rapidly. Diagnosis involves slit lamp examination, staining, and cultures of corneal scrapings.
![Slit
lamp
examina
tion of
cornea
Epithelium, including defects and punctate keratopathy, oedema, epithelial
movement patterns.
Stroma, including ulceration, thinning, perforation, and infiltrate (location -central,
peripheral, inferior, perineural, surgical, or traumatic wound), density, size, shape
[ring], number [satellite], depth, character of infiltrate margin [suppuration,
necrosis, feathery, soft, crystalline], color), oedema.
Endothelium (endothelial plaque)
Foreign body, including sutures.
Signs of corneal dystrophies (e.g., epithelial basement membrane dystrophy)
Previous corneal inflammation (thinning, scarring, or neovascularization)
Signs of previous corneal or refractive surgery
Ref. AAO PPP Cornea/External
Disease Committee, Hoskins Center
for Quality Eye Care
Cornea/External Disease
17](https://image.slidesharecdn.com/bacterialkeratitis-200626023613/85/Bacterial-keratitis-17-320.jpg)









































![keratitis [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/keratitisautosaved-220807175619-8bc9d2cd-thumbnail.jpg?width=640&height=640&fit=bounds)








































