








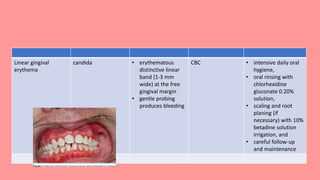
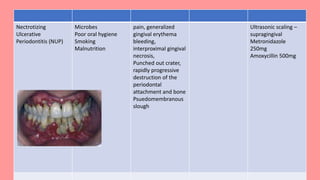



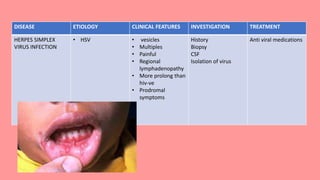




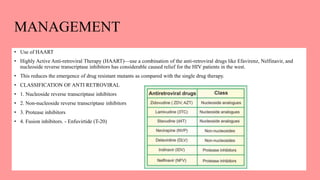



The document provides an extensive overview of human immunodeficiency virus (HIV) infection and acquired immune deficiency syndrome (AIDS). It covers the virus's epidemiology, structure, classification, modes of transmission, phases of infection, oral manifestations, and diagnostic methods. The document also details the clinical features, potential complications, and treatment approaches associated with HIV-related illnesses.



































































