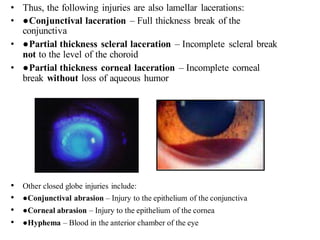
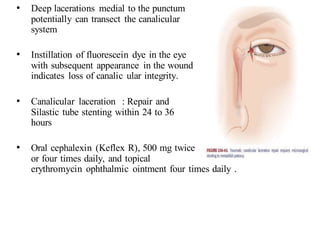
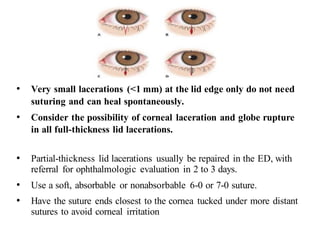
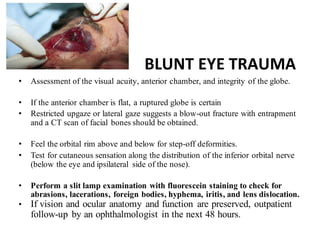
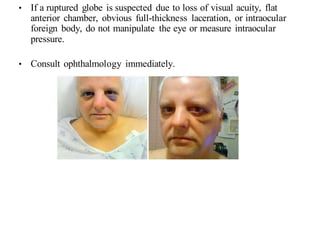
The document discusses various types of ocular injuries including open globe injuries, closed globe injuries, and periocular injuries. Open globe injuries involve a full thickness break of the eye wall, while closed globe injuries do not penetrate the full thickness. Periocular injuries involve structures surrounding the eye such as the eyelids. Specific injuries like corneal abrasions, hyphema, and lid lacerations are described along with their typical presentations, evaluations, and treatments. Ocular trauma requires careful examination and many cases need referral to an ophthalmologist.