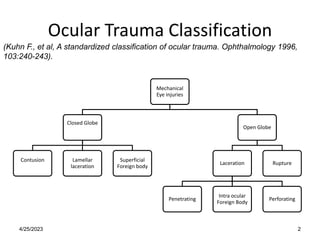
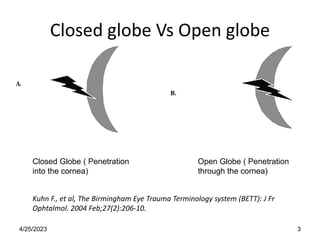
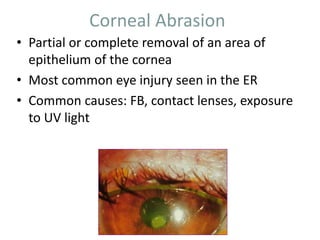
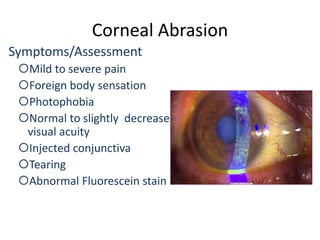
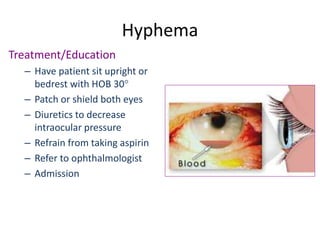
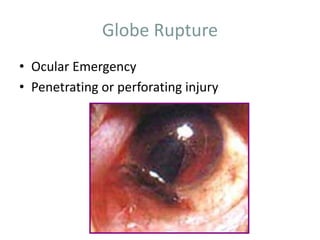
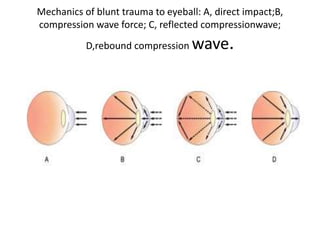
This document discusses various types of ocular trauma including classification, symptoms, assessment, diagnostics, and treatment. It covers closed and open globe injuries, corneal abrasions, extraocular foreign bodies, orbital fractures, hyphema, eyelid lacerations, globe ruptures, and chemical burns. Common injuries from blunt trauma include commotio retinae, retinal hemorrhages, choroidal ruptures, and vitreous hemorrhage or detachment. Assessment examines mechanism of injury and complications involving iris, lens, vitreous, choroid, and retina. Treatment priorities are irrigation, antibiotics, patching, referral to ophthalmologist, and surgery if needed to repair damage and prevent complications.