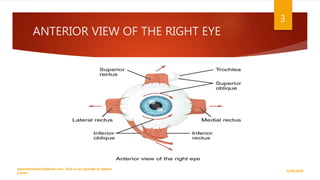
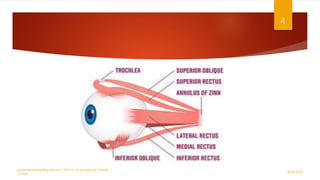
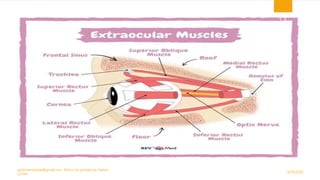
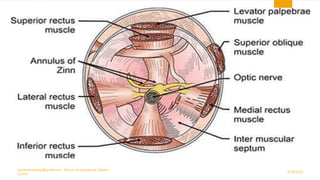
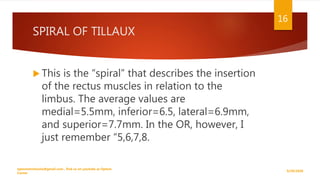
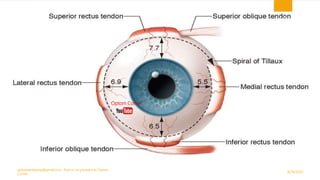
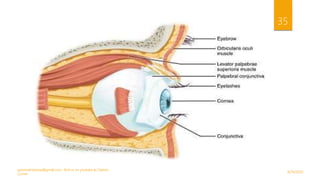
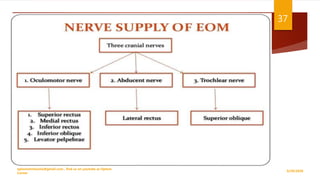
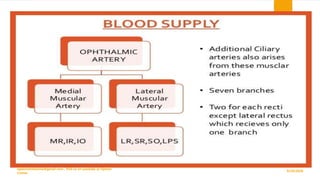
The document discusses the extraocular muscles (EOM) that control eye and eyelid movement. It describes the six muscles responsible for eye movement - the four rectus muscles (superior, inferior, medial, lateral) and two oblique muscles (superior, inferior). It also discusses the levator palpebrae superioris muscle responsible for raising the upper eyelid. The origins, insertions, innervations and actions of each muscle are defined.