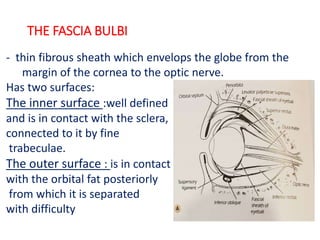
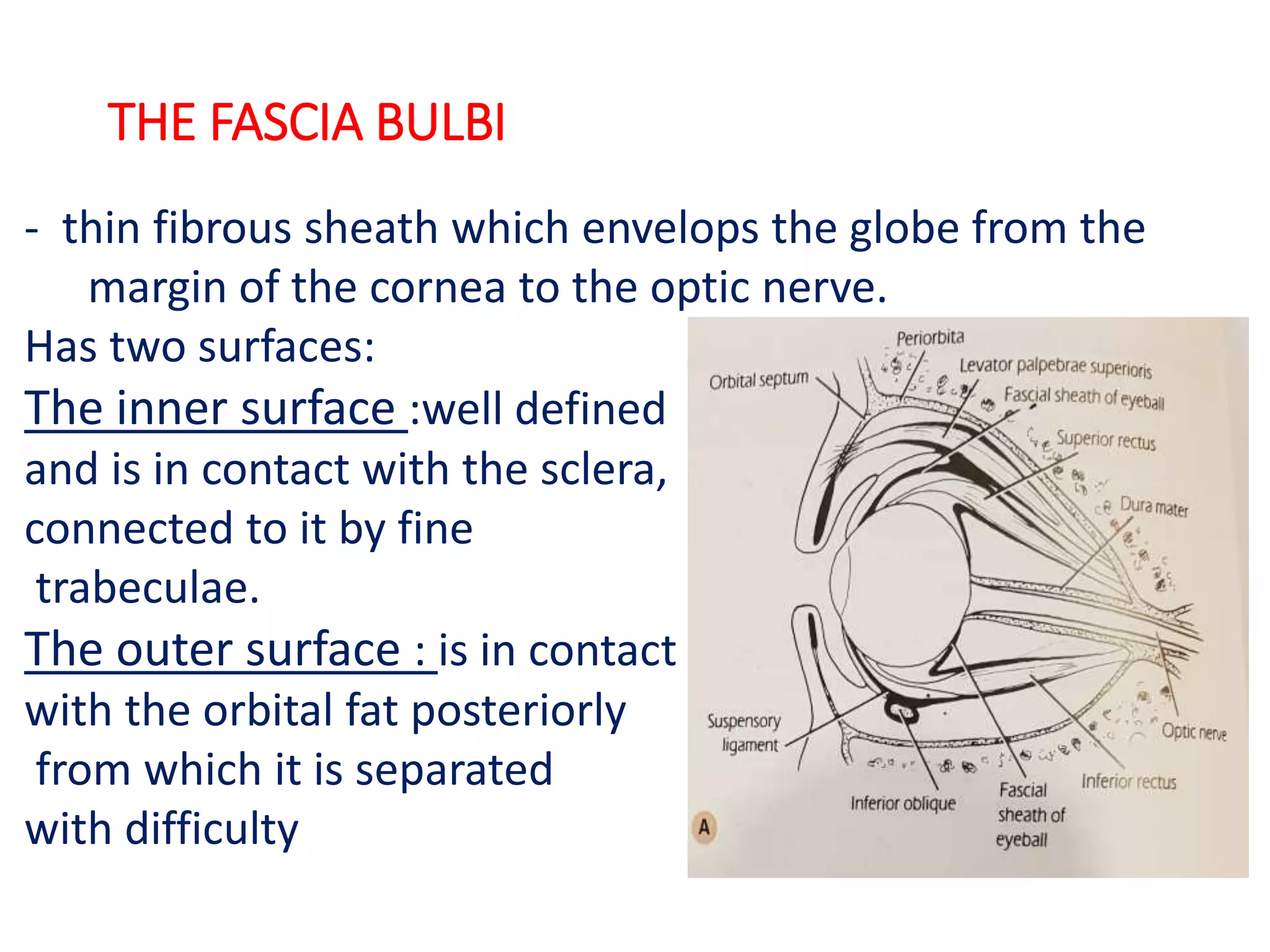
The fascia bulbi is a thin fibrous sheath that envelops the globe from the cornea to the optic nerve. It has two surfaces - an inner surface firmly attached to the sclera, and an outer surface in contact with the orbital fat. Its main functions are to position and support the globe within the orbital cavity and allow movements of the extrinsic eye muscles. It is important during eye surgery and enucleation to preserve the fascia bulbi to serve as a socket for a prosthesis.