This document provides information on occupational lung diseases. It begins with a brief history of occupational lung diseases dating back to Roman times. It then defines occupational lung diseases and pneumoconiosis. The document classifies and describes various types of pneumoconiosis including anthracosis, silicosis, asbestosis, and berylliosis. For each type, it discusses associated occupations, pathogenesis, clinical features, diagnosis, and management. The document provides detailed information on the pathogenesis, clinical presentation, radiographic findings, and complications of major occupational lung diseases like silicosis and asbestosis.

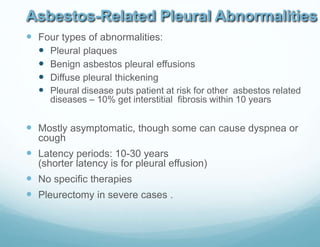
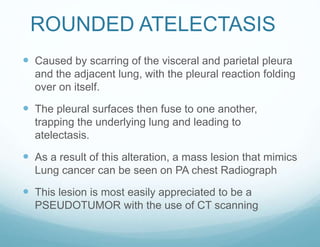
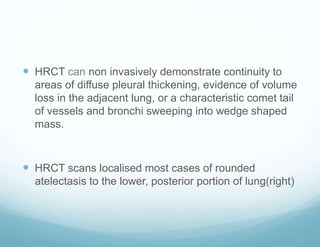
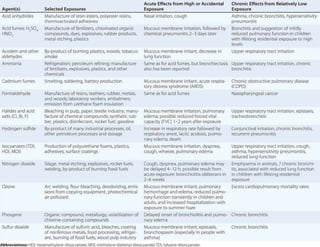
![ Clinical forms:
Acute silicosis- it develops with 10 months of silica
exposure
Clinical and pathologic features are similar to
pulmonary alveolar proteinosis .It is a quite severe
form and is progressive despite discontinuation of
exposure.
Xray - chest - profuse miliary infiltration or
consolidation,
No silicotic nodules
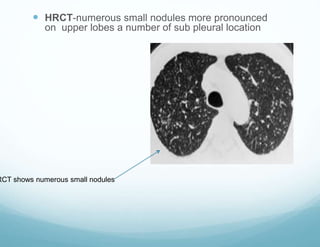
HRCT- characteristic pattern-Crazy paving [thickened
intra and interlobar septa producing polygonal shapes
].
Treatment- whole lung lavage provide symptomatic
relief](https://image.slidesharecdn.com/occupationallungdisease-160423173406-190419102504/85/Occupationallungdisease-160423173406-31-320.jpg)
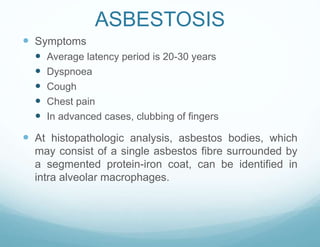
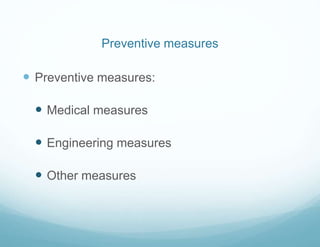
![Asbestos-related diseases
Benign
Pleural diseases
1.plaques
2.diffuse pleural thickening
3.effusion
4.calcification
Parenchymal diseases
1.Asbestosis [parenchymal
fibrosis caused by asbestos
inhalation]
2.Rounded atelectasis
3.Benign fibrotic masses
4.Transpulmonary bands
Malignancy
1.Malignant mesothelioma
2.Bronchogenic carcinoma](https://image.slidesharecdn.com/occupationallungdisease-160423173406-190419102504/85/Occupationallungdisease-160423173406-42-320.jpg)
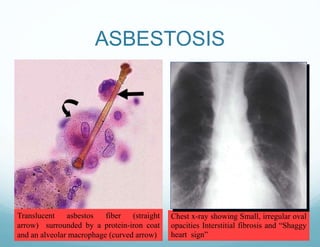
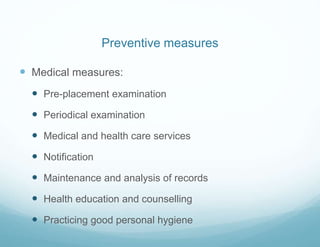
![ Clinical features- cough , chest pain, arthralgia's
,fatigue and weight loss
BeLPT[beryllium lymphocyte proliferation test ]-blood is
drawn and in the lab, the WBC are separated from the rest
of the blood cells and then mixed with beryllium solution. If
the immune system is sensitized to beryllium, the cells will
multiply, producing an abnormal BeLPT result.In normal
individuals cells will not multiply.
Fiberoptic bronchoscopy with transbronchial lung biopsy is
required to make diagnosis of CBD . Biopsy shows
noncaseating granulomas or monocytic infiltration in lung
tissue.](https://image.slidesharecdn.com/occupationallungdisease-160423173406-190419102504/85/Occupationallungdisease-160423173406-55-320.jpg)




























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















