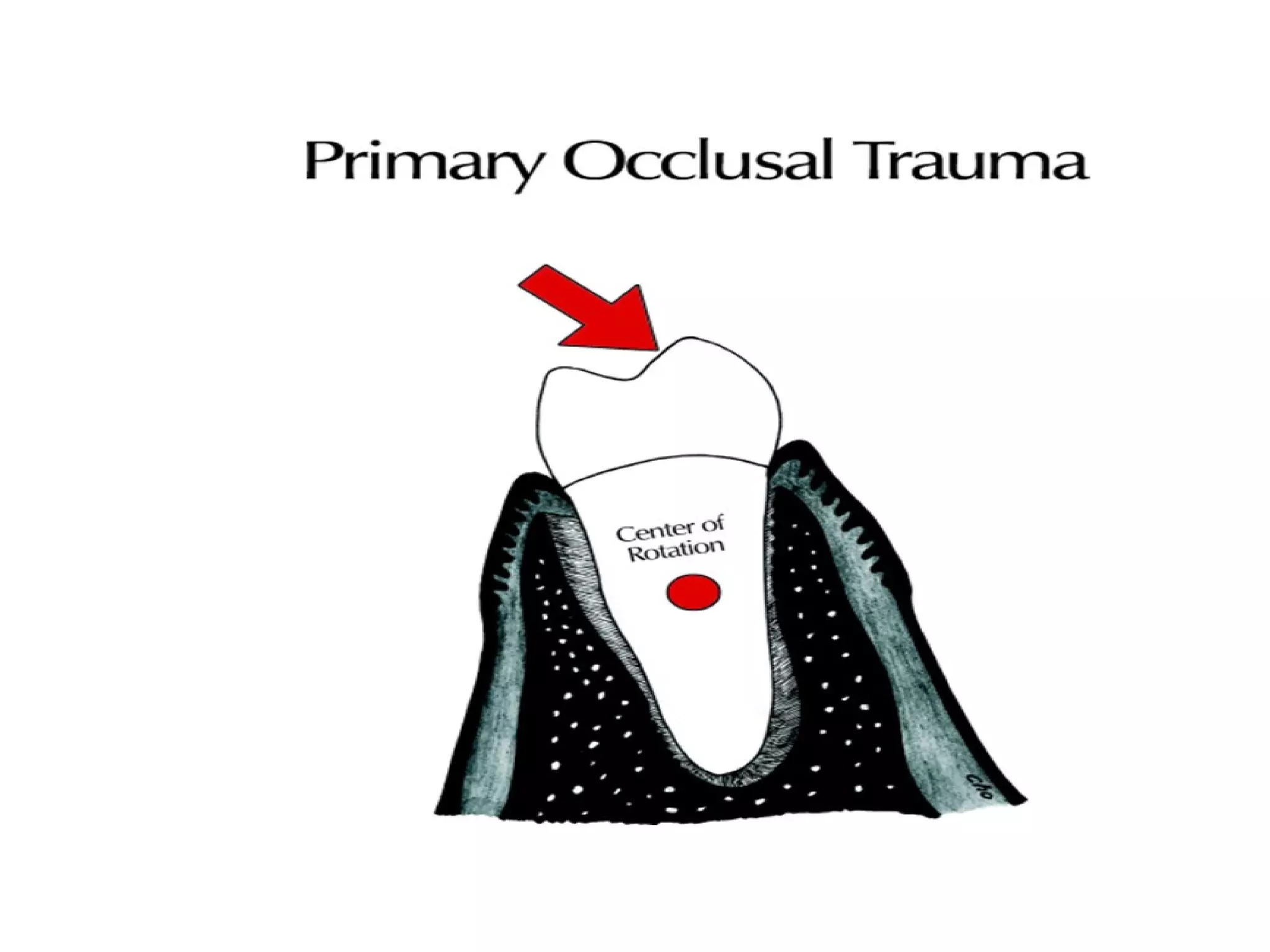
This document defines and describes primary and secondary occlusal trauma, which are injuries to the periodontium resulting from excessive occlusal forces. Primary trauma occurs with normal bone and attachment levels, while secondary trauma occurs with bone or attachment loss. Histological studies in animals and humans show that occlusal forces can cause widening of the periodontal ligament space, bone remodeling, root resorption, and other changes depending on the force magnitude and direction. Clinical indicators include tooth mobility, occlusal prematurities, sensitivity, and radiographic changes like widening of the periodontal ligament space. Diagnosis involves examining history, teeth for attrition, decreased vertical dimension, and radiographs. Treatment may include extra























![Treatment;
not every trauma from occlosion require treatment
just keep these patient under observation.
We should not change the pattern of occlusion
unless we are sure that pattern is causing the
problem.
For example; sometimes the cause is the
muscles[uncoordinated] so no matter how much
we trim the teeth we wont solve the problem.](https://image.slidesharecdn.com/occlusaltrauma-131015145745-phpapp01/75/Occlusal-trauma-26-2048.jpg)


![Treatment;
1-interfering hopeless tooth-extraction.
2-new restoration of interfering teeth.
3-diminshed occlusal table require placement [bridge,partial denture….]
4-bite plane,night guard,now called [inter-occlusal appliance]
a-prevent teeth from fully interdigitating.
b-help in preventing or minimizing isomeric contraction of muscles.
c-abolish the effect of mechanoreceptors.
5-exercise for more harmonious occlusion.
6-portable electromyography contain warning system[feed back] measures the electric potential on the
muscles.](https://image.slidesharecdn.com/occlusaltrauma-131015145745-phpapp01/75/Occlusal-trauma-29-2048.jpg)












































































