
Recommended
More Related Content
What's hot
What's hot (20)
Similar to The Periodontal Pocket
Similar to The Periodontal Pocket (20)
Recently uploaded
Recently uploaded (20)
The Periodontal Pocket
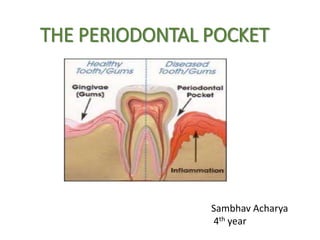
- 1. THE PERIODONTAL POCKET Sambhav Acharya 4th year
- 2. OUTLINE DEFINITION CLASSIFICATION CLINICAL FEATURES PATHOGENESIS HISTOPATHOLOGY CONTENTS OF POCKET DETECTION OF POCKET MANAGEMENT REFERENCE
- 3. • The periodontal pocket is defined as a pathologically deepened gingival sulcus • It is one of the most important clinical features of periodontal disease
- 4. •Deepening of the gingival sulcus may occur by coronal movement of the gingival margin , apical displacement of the gingival attachment or a combination of the both
- 5. Pockets can be classified as follows: a) Gingival pocket (pseudo pocket) : This type of pocket is formed by the gingival enlargement without destruction of the underlying periodontal tissues . The sulcus is deepened because of the bulk of the gingiva b) Periodontal pocket : This type of pocket occurs with the destruction of the supporting periodontal tissues. 2 types of periodontal pocket exist, as follows • Suprabony (supracrestal, supraalveolar), in which the bottom of the pocket is coronal to the underlying alvelor bone • Intrabony (infrabony ,subcrestal,intralveolar) , in which the bottom of the pocket is apical to the level of the adjacent alvelor bone. The lateral pocket wall lies between the tooth surface and the alveolar bone.
- 6. Fig : Different types of periodontal pockets
- 7. It can also be classified as 1. According to the involved tooth surface a) Simple pocket • Involves one surface b) Compound pocket • Involves more than one surface c)Complex pocket (spiral) • Originating on one tooth surface and twisting around the tooth to involve one or more additional surfaces • Most common in furcation areas
- 8. 2.Depending upon the nature of the soft tissue wall • Edematous pocket • Fibrotic pocket 3.Depending upon the disease activity • Active pocket • Inactive pocket
- 9. Clinical Features Enlarged, bluish-red marginal gingiva “rolled” edge Reddish blue vertical zone Extrusion & migration diastema shiny & puffy gingiva gingival bleeding purulent exudate
- 10. (B) SYMPTOMS •Localized pain or pain “ deep in the bone” •Usually painless but may give rise to the localized/radiating pain or sensation of the pressure after eating which gradually decreases •Sensitivity to hot and cold fluid •Tooth may become loose •Feeling of itching in the gums
- 11. Correlation of clinical and histopathologic features of periodontal pocket Clinical features Gingival wall of pocket presents various degrees of bluish red discoloration Flaccidity A smooth shiny surface and pitting on pressure Bleeding is elicited on gentle probing soft tissue wall of pocket Gingival wall – pink & firm Histopathologic features Discoloration caused by circulatory stagnation Destruction of gingival fibers and surrounding tissues Atrophy of epithelium and edema & the pitting on pressure by edema and degeneration Results from the increased vascularity, thinning and degeneration of epithelium and proximity of engorged vessel to inner surface Fibrotic changes predominate over exudation and degeneration
- 12. PATHOGENESIS The initial lesion in the development of periodontitis is the inflammation of gingiva in response to a bacterial challenge Changes involved in transition from the normal gingival sulcus to the pathological periodontal pocket are associated with different proportions of bacterial cells in dental plaque Pocket formation starts as an inflammatory change in the connective tissue wall of the gingival sulcus Cellular and fluid inflammatory exudates causes degeneration of the surrounding connective tissue including gingival fibers Just apical to the junctional epithelium, collagen fibers are destroyed And the areas become occupied by inflammatory cells and edema
- 13. PMNLs and macrophages secreted by various cells become extracellular and destroy collagen fibers in gingival CT .These enzyme that degrade collagen into small peptide are called matrix metalloprotinases Fibroblast phagocytize fibers by extending cytoplasmic process to the ligament cementum interface and degrade the collagen fibers of the cementum matrix Collagen loss is caused by 2 mechanisms
- 14. After collagen loss, apical cells of Junctional epithelium proliferate along the root, extending finger like projections two or three cells in thickness Coronal portion of Junctional Epithelium detaches from roots as apical portion migrates. As a result of inflammation PMNs invades coronal end of Junctional Epithelium in increasing number and when relative volume of PMNs becomes approx. 60% or more of Junctional Epithelium, tissue looses cohesiveness & detaches from tooth surface.
- 15. The transformation of a gingival sulcus into a pocket creates an area where plaque removal becomes impossible and feedback mechanism is established Plaque accumulation Gingival inflammation Pocket formation Area difficult to clean
- 16. Histopathology Once the pocket is formed several microscopic features are present: Soft tissue wall The connective tissue is edematous and densely infiltrated with the plasma cells(approx 80%),lymphocytes, and scattering of PMNs The blood vessels are increased in number, dilated and engorged The connective tissue exhibits varying degrees of degeneration Single or multiple necrotic foci are present The connective tissue also shows the proliferation of the endothelial cells with the newly formed capillaries, fibroblast, and collagen fibers
- 17. Junctional epithelium : coronoapical length reduced to 50 -100ɱm Cells : well formed & in good condition Slight to marked degeneration Connective tissue:
- 18. Lateral wall Most severe degenerative changes Epithelial buds or interlacing cords of epithelial cells project from the lateral wall into the adjacent inflamed connective tissue Dense infiltration Cells : vacuolar degeneration & rupture to for vesicles Ulceration and suppuration
- 19. Fig 1: Lateral wall showing epithelial proliferation and atrophic changes Fig2: Base of the pocket showing extensive proliferation of lateral epithelium
- 20. Bacterial invasion • Filaments , rods and coccoid organism with predominant gram- negative cell walls have been found in intercellular spaces of the epithelium • Bacteria may invade the intercellular space under exfoliating epithelial cells<but they are also found between deeper epithelial cells and accumulating on the basement lamina. Some bacteria transverse the basement lamina and invade the sub epithelial connective tissue
- 21. Microtopography of Gingival wall Scanning electron microscopy has permitted the description of several areas in the soft tissue wall of periodontal pocket. Seven different type of disease activity have been noted 1. Area of relative quiescence : Region with minor depressions and elevation 2. Areas of bacterial accumulation : accumulates in depression of epithelial cells
- 22. 4.Areas of leukocytes-bacteria interaction: where numerous leukocytes are present and covered with bacteria in an apparent process of phagocytosis 5.Areas of intense epithelial desquamation 6.Areas of hemorrhage 7.Areas of ulceration 3.Areas of emergence of leukocytes : leukocytes emerging through intercellular space
- 23. Periodontal pocket as a healing lesion Periodontal pocket are chronic inflammatory lesions and thus are constantly undergoing repair Complete healing doesn’t occur because of the persistence of the bacterial attack which continues to stimulate an inflammatory response causing degeneration of the new tissue element FIBROTIC POCKET WALL: When the reparative changes predominate , the gingiva appear fibrotic & pink
- 24. EDEMATOUS POCKET WALL : When the inflammatory fluid and the cellular exudates predominates, the lateral wall appears bluish red, soft, spongy and friable with a smooth shiny surface referred to as an edematous pocket wall
- 25. CONTENTS OF A POCKET • Debris ( consisting of microorganism & their product mainly enzymes, toxin and other metabolic products) • Gingival fluid • Food remnants • Salivary mucin • Desquamated epithelial cells & leukocytes Plaque covered calculus projects from the tooth surface • If purulent exudates present: consist of living, degenerated and necrotic leukocyte, living and dead bacteria ,Serum • Scant amount of fibrin
- 26. SIGNIFICANCE OF PUS FORMATION Pus is a common feature of periodontal disease, but it is only a SECONDARY SIGN It is NOT AN INDICATION OF THE DEPTH OF THE POCKET or the severity of the destruction of the supporting tissues
- 27. ROOT SURFACE WALL Undergoes following changes: STRUCTURAL CHEMICAL CYTOTOXIC
- 28. RUCTURAL CHANGES Exposure of cementum to the oral environment Mineral present in saliva tend to get deposited in cementum surface Areas of hypermineralization Root surface is exposed to oral fluids and bacterial plaque Proteolysis of embedded remnants of sharpeys fiber Root caries( yellowish or light brown patch) soft and lethargy on probing Patient feels severe sensitivity to thermal changes and sweet pulp exposure may occur in severe forms
- 29. CHEMICAL CHANGES • Mineral content increased • Fluoride, Calcium, Magnesium, Phosphorus • Exposed cementum : Resistant to decay CYTOTOXIC CHANGES • histological studies of the periodontally involved cementum shows the presence of bacteria in the cementum or the endotoxin in the cementum
- 30. SURFACE MORPHOLOGY OF TOOTH WALL Five zones can be seen on the base of the pocket (1) Cementum covered by calculus (2) Attached plaque (3) Zone of unattached plaque (4) Zone of attachment of the junctional epithelium to the tooth (5) Zone of semi destroyed connective tissue fibers
- 31. PERIODONTAL DISEASE ACTIVITY • Periodontal pocket go through the periods of exacerbation and quiescence PERIODS OF QUIESCENCE •REDUCED INFLAMMATORY RESPONSE • LITTLE OR NO LOSS OF BONE AND CONNECTIVE TISSUE ATTACHMENT PERIODS OF EXACERBATION •BONE AND CONNECTIVE TISSUE ATTACHMENT ARE LOST AND THE POCKET DEEPENS •BLEEDING EITHER SPONTANEOUSLY OR WITH PROBING •GREATER AMOUNT OF GINGIVAL EXUDATE
- 32. Detection of pocket The only accurate method for detecting and measuring periodontal pockets is careful exploration with periodontal probe Disadvantage of a radiograph • Pocket is a soft tissue change. • Radiograph indicate areas of bone loss where pockets may be suspected. •They don’t show pocket presence or depth, and consequently they show no difference before and after pocket elimination unless bone loss has been modified.
- 33. Pocket probing Two probing depths present (A) Biologic or histologic depth : it is the distance between gingival margin and the base of the pocket ( the coronal end of junctional epithelium) (B) Clinical or probing depth :it is the distance from the gingival margin to which a probe penetrates into the pocket The probing force of 0.7 N or 25gm have been found to be well tolerated or accurate
- 34. Pocket depth versus Attachment loss • Pocket depth : Distance between base of pocket & the gingival margin • Level of attachment loss : Distance between the base of the pocket and the fixed point on a crown such as CEJ
- 35. ‘WALKING’ the probe to explore the entire pocket Probing technique Vertical insertion of the probe (left) may not detect interdental craters ,oblique positioning of the probe(right) reaches the depth of the crater
- 37. Management of pocket • NON- SURGICAL MANAGEMENT : including a) phase I therapy b)local drug delivery c)systemic antimicrobials • SURGICAL MANAGEMENT : including a) Resective surgeries Gingival curettage Gingivectomy periodontal Flap procedue b) Regenerative surgeries
- 38. CONCLUSION • Periodontal pocket is defined as pathologically deepened gingival sulcus • Deepening of the gingival sulcus may occur by coronal movement of the gingival margin , apical displacement of the gingival attachment or a combination of the both •Periodontal pocket is classified depending upon morphology ,nature of soft tissue wall, involved tooth surface and disease activity •The clinical features seen in periodontal pockets are correlated with the histological features • Detection and treatment of periodontal pocket is important as it starts as a first step in the periodontal breakdown