Downloaded 757 times













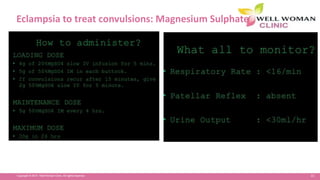

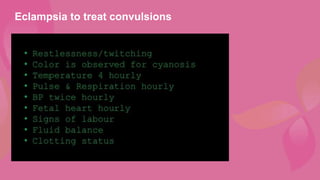
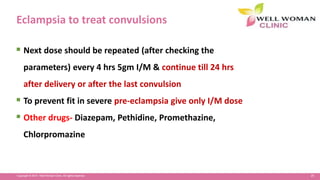

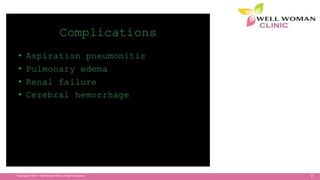

























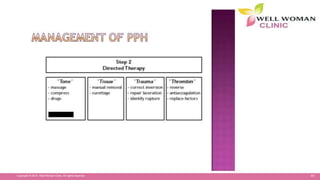














The document discusses various obstetric emergencies including hypertensive disorders of pregnancy like preeclampsia and eclampsia. It describes complications in each trimester such as ectopic pregnancy, abortion, and postpartum hemorrhage. It provides details on the management of preeclampsia including delivery within 12 hours of onset of convulsions. Magnesium sulfate is discussed as the treatment for eclampsia. Risk factors, signs, and management of obstetric emergencies like abruptio placentae, placenta previa, and postpartum hemorrhage are also summarized.




































![maternal guide presentation [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/maternalpresentationautosaved-250208125838-a01bbc1b-thumbnail.jpg?width=640&height=640&fit=bounds)

















![Vitamin D and Women's Health [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/vitamindwomenhealthautosaved-191231021803-thumbnail.jpg?width=640&height=640&fit=bounds)
































