INTRODUCTION –
Obstetric emergenciesare health problems that are life-threatening
for pregnant women and their babies. An obstetric emergency may
arise at any time during pregnancy, labour and birth. Hospital care is
needed for all obstetric emergencies, as the woman may need
specialist care and an extended hospital stay.
DEFINITION
Obstetrical emergencies are life-threatening medical conditions that
occur in pregnancy or during or after labour and delivery
4.
Cord isprolapse
Retained second twin
Severe anaemia in pregnancy
Cord presentation
Uterine inversion
COMMON OBSTETICAL EMERGENCY
Prolonged labour
Obstructed labour
Postpartum haemorrhage
Fetal distress
Severe pregnancy-induced hypertension
Eclampsia
Antepartum haemorrhage
Puerperal sepsis
Ruptured uterus
5.
1. OBSTETRICS EMERGENCYDURING PREGNANCY
Obstetrics emergencies that may arise during pregnancy include
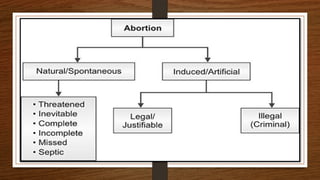
a. ABORTION/MISCARRIAGE
Abortion is also k/a miscarriage
Abortion is the ending of pregnancy By removing a fetus or embryo Before it can survive outside the
Uterus, if the fetus or wt is less than 500gm at 20 weeks of gestation. The expelled embryo or fetus is
called abortion.
It may be induced or spontaneous. In India about 6 million abortion are take place, 2 million abortion
are spontaneous and 4 million Induced.
38,000 death from unsafe abortion unusually World wide...
6.
Cause:
Maternal cause
1.Maternal infection
2.Maternaldisease
3. Drug
2. Hormonal disturbance
Fetal cause
Chromosomal anomalies
Congenital defect
Hydatiform mole
Blighted ovum
Other cause
Uterine developmental anomalies
Retroversion Fibromyoma of uterus
Surgery during pregnancy.
Environmental factors-cigarette, alcohol Immune factors-
Rh-ve blood
8.
THREATENED ABORTION:
Itis a clinical entity where choriodecidual Haemorrhage has begun, but not progressed To the stage of
irreversibility, this means the Cervix is not open and the product of concept -ion, are not expelled .Baby
survival is possible
Sign and symptoms:-painless vaginal bleeding without uterine contraction, cervix is soft.
Diagnostic Evaluation:-blood,urine,usg, thyroid FT.
Treatment:- HRT,HCG inj.,Analgesic....
INEVITABLE ABORTION:
In this type of abortion the process has begun $ progressed to such an extent that expulsion Of the product of
conception seems inevitable Continuation of pregnancy is impossible.
Sign and symptoms:- vaginal bleeding with clot or product of Conception.
Diagnostic Evaluation:- History collection, vaginal exam. ,blood, USG,
Treatment:-less than 12 weeks -suction evacuation more than 12 weeks -oxytocin 10unit 500ml NS
9.
INCOMPLETE ABORTION
Inspite of uterine contractions and cervical dilatation, only the fetus and some membranes arg expelled .
The placenta remains partly attached and bleeding continue
This abortion must be completed by surgical methods
COMPLETE ABORTION
When the products of conception are completely expelled, it is called complete abortion.
NURSING MANAGEMENT:
Preoperative care:-- Postoperative care :--
Health education :
DIET :-fresh fruits pulses, cereals, wholes Avoid smoking ,refined food.
EXERCISE:- Avoid heavy work and heavy exercise
HYGIENE:- maintain perineal hygiene.
10.
MEDICAL TERMINATION OFPREGNANCY ACT (1971):
MTP is a medical termination of pregnancy .Its also known as induced
abortion .It is the medical way to getting rid of Unwanted pregnancy.
The termination of a pregnancy by the removal or expulsion of an embryo or fetus from the uterus..
11.
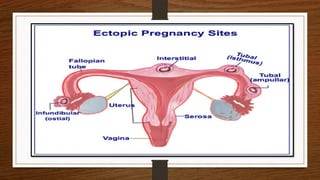
a. ECTOPIC PREGNANCY–
An ectopic pregnancy is one where implantation occurs at a site other than the uterine cavity. Sites
can be in the uterine tube, ovary, cervix and the abdomen
About 1% of all pregnancies are ectopic and the life threatening outcome of this condition calls for
appropriate treatment for the mother.
Any alteration of the normal function of the uterine tube in transporting the gametes contributes to the
risk of tubal pregnancy:
Inflammation and scarring of the fallopian tubes from a previous medical condition, infection, or
surgery.
Hormonal factors
Genetic abnormalities or congenital abnormalities
Medical conditions that affect the shape and condition of the fallopian tubes and hormonal factors
13.
Sign and symptoms
sharp waves of pain in the abdomen, pelvis, shoulder, or neck
severe pain that occurs on one side of the abdomen
light to heavy vaginal spotting or bleeding
dizziness or fainting
rectal pressure
Medical management
The most common drug used to treat ectopic pregnancy is methotrexate. This drug stops cells
from growing, which ends the pregnancy. The pregnancy then is absorbed by the body over 4–6
weeks. This does not require the removal of the fallopian tube.
Surgical treatment–
Salpingectomy and salpingectomy are two laparoscopic surgeries used to treat some ectopic
pregnancies.
14.
Complications
An ectopic pregnancycan cause your fallopian tube to burst open. Without treatment,
the ruptured tube can lead to life-threatening bleeding.
Prevention
There's no way to prevent an ectopic pregnancy, but here are some ways to decrease your
risk:
Limiting the number of sexual partners and using a condom during sex helps to prevent
sexually transmitted infections and may reduce the risk of pelvic inflammatory disease.
Don't smoke. If you do, quit before you try to get pregnant.
15.
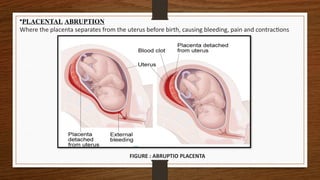
•PLACENTAL ABRUPTION
Where theplacenta separates from the uterus before birth, causing bleeding, pain and contractions
FIGURE : ABRUPTIO PLACENTA
16.
ClassificationRevealed type: Bleedingis revealed.
Concealed type: No obvious bleeding.
Mixed type: Combination of 1&2 above.
In the concealed type(20%), the haemorrhage is confined within the uterine cavity,
detachment of the placenta may be complete, and the complications are often severe.
In the revealed type(80%) the blood drains through the cervix, placental detachment is more
likely to be incomplete, and the complications are fewer and less severe
17.
Management
1. Fluid andblood replacement.
2. Vaginal delivery if bleeding is minimal, the mother's condition is stable, the labor is progressing
and the presenting part is in the pelvis. Labour may have to be augmented (induced) if it is not
progressing well.
3. Cesarean delivery if haemorrhage is severe, fetal heart tones are present, the presenting part is
not in the pelvis, the cervix is closed or if it is anticipated that birth is not imminent.
If he fetus is dead, a cesarean section is performed only if the bleeding is life-threatening. A cesarean
hysterectomy may be necessary if the bleeding cannot be controlled
18.
Possible Complications
1. Severeshock may cause renal failure with first hematuria, then oliguria or anuria due
to necrosis of the nephrons.
2. Coagulation defect, if not treated successfully can lead to catastrophic bleeding due
to disseminated intravascular coagulation (DIC)
3. .Heavy blood loss and shock can cause pituitary necrosis leading to Sheehan's
syndrome.
4. Postpartum haemorrhage may occur as a result of the couvelaire uterus and DIC.
19.
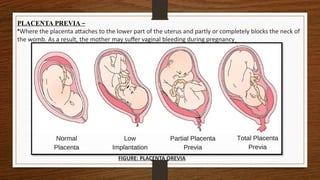
PLACENTA PREVIA –
•Wherethe placenta attaches to the lower part of the uterus and partly or completely blocks the neck of
the womb. As a result, the mother may suffer vaginal bleeding during pregnancy
FIGURE: PLACENTA OREVIA
20.
Etiology
These vessels maybe from either
Velamentous insertion of umbilical cord
placental lobe joined to the main disk of the placenta.
Low-lying placement
Previous delivery by C-section.
Symptoms
The baby's blood is a darker red colour due to lower oxygen levels of a fetus
Sudden onset of painless vaginal bleeding, especially in their second and third
trimesters
If very dark burgundy blood is seen when the water breaks, this may be an indication
of vasa
21.
Management
Antepartum
The patientshould be monitored closely for preterm labor, bleeding or rupture
of membranes.
Steroids should be administered at about 32 weeks.
Hospitalization at 32 weeks is reasonable.
Take patient for emergency caesarean section if
membranes are ruptured.
Fetal growth ultrasounds should be performed at least every 4 weeks.
Cervical length evaluations may help in assessing the patient's risk for preterm
delivery or rupture of the membranes
22.
should not beallo Intrapartum
The patient wed to labour. She should be delivered by elective caesarean at about 35 weeks
Delaying delivery until after 36 weeks increases the risk of membrane rupture.
Care should be taken to avoid incising the fetal vessels at the time of caesarean delivery.
If vasa Previa is recognized during labour in an undiagnosed patient, she should be delivered by
urgent caesarean. The placenta should be examined to confirm the diagnosis
Postpartum
Routine postpartum management as for cesarean delivery.
If the fetus is born after blood loss, transfusion of blood without delay may be life-saving.
It is important to have O negative blood or type-specific blood available immediately for neonatal
transfusion
23.
Nursing Management
Assessbleeding, colour, amount
Administer iv fluids.
Administer oxygen.
Strict vitals and FHS monitoring.
Prepare patient for caesarean section. o Reserve blood if (Hct
>30%)
24.
a. PRE-ECLAMPSIA
Pre-eclampsia (orpregnancy-induced high blood pressure) causes severe swelling from water retention. It can to
kidney and liver failure. If it progresses to eclampsia (convulsions), it can be fatal for the mother and her baby
Preeclampsia is a multisystem disorder of unknown etiology characterized by development of hypertension to the
extent of 140/90 mm Hg or more with proteinuria induced by pregnancy after the 20th week in a previously
normotensive and non-proteinuria woman (International Society for Study of Hypertension in Pregnancy, 1988
Incidence
About 5-8% of all pregnancies are complicated by hypertension and of these preeclampsia accounts for 80%
(Llewellyn Jones, 1990). It occurs more frequently in young primigravida and in mothers over 35 years of age. It
is known to be associated with hydatidiform mole, multiple pregnancy and maternal diabetes.
25.
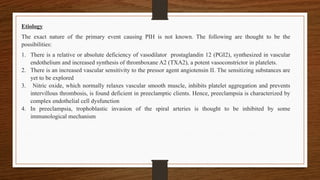
Etiology
The exact natureof the primary event causing PIH is not known. The following are thought to be the
possibilities:
1. There is a relative or absolute deficiency of vasodilator prostaglandin 12 (PGI2), synthesized in vascular
endothelium and increased synthesis of thromboxane A2 (TXA2), a potent vasoconstrictor in platelets.
2. There is an increased vascular sensitivity to the pressor agent angiotensin II. The sensitizing substances are
yet to be explored
3. Nitric oxide, which normally relaxes vascular smooth muscle, inhibits platelet aggregation and prevents
intervillous thrombosis, is found deficient in preeclamptic clients. Hence, preeclampsia is characterized by
complex endothelial cell dysfunction
4. In preeclampsia, trophoblastic invasion of the spiral arteries is thought to be inhibited by some
immunological mechanism
26.
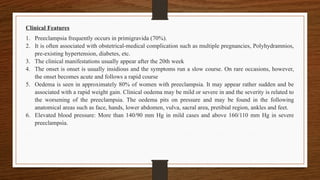
Clinical Features
1. Preeclampsiafrequently occurs in primigravida (70%).
2. It is often associated with obstetrical-medical complication such as multiple pregnancies, Polyhydramnios,
pre-existing hypertension, diabetes, etc.
3. The clinical manifestations usually appear after the 20th week
4. The onset is onset is usually insidious and the symptoms run a slow course. On rare occasions, however,
the onset becomes acute and follows a rapid course
5. Oedema is seen in approximately 80% of women with preeclampsia. It may appear rather sudden and be
associated with a rapid weight gain. Clinical oedema may be mild or severe in and the severity is related to
the worsening of the preeclampsia. The oedema pits on pressure and may be found in the following
anatomical areas such as face, hands, lower abdomen, vulva, sacral area, pretibial region, ankles and feet.
6. Elevated blood pressure: More than 140/90 mm Hg in mild cases and above 160/110 mm Hg in severe
preeclampsia.
27.
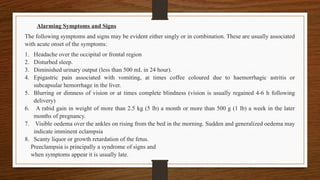
Alarming Symptoms andSigns
The following symptoms and signs may be evident either singly or in combination. These are usually associated
with acute onset of the symptoms:
1. Headache over the occipital or frontal region
2. Disturbed sleep.
3. Diminished urinary output (less than 500 mL in 24 hour).
4. Epigastric pain associated with vomiting, at times coffee coloured due to haemorrhagic astritis or
subcapsular hemorrhage in the liver.
5. Blurring or dimness of vision or at times complete blindness (vision is usually regained 4-6 h following
delivery)
6. A rabid gain in weight of more than 2.5 kg (5 lb) a month or more than 500 g (1 lb) a week in the later
months of pregnancy.
7. Visible oedema over the ankles on rising from the bed in the morning. Sudden and generalized oedema may
indicate imminent eclampsia
8. Scanty liquor or growth retardation of the fetus.
Preeclampsia is principally a syndrome of signs and
when symptoms appear it is usually late.
Effects on theFetus
1. Reduced placental function can result in low birth weight.
2. There is an increased incidence of hypoxia in both the antenatal and intrapartum
period.
3. Placentae fetal hypoxia; if major, intrauterine death will occur.
4. Early delivery, if the disease worsens or if abruption occurs, which will produce a
preterm baby requiring resuscitation
Complications
Immediate
1. During pregnancy:
Eclampsia 2% (more in acute cases)
Placental abruption and intrauterine fetal death
Oliguria and anuria - Dimness of vision and
blindness - Preterm labour - Hemolytic anaemia, elevated
liver enzymes, low platelet count (HELLP) syndrome
30.
2. labour –
Eclampsia
Postpartum hemorrhage may be related with coagulation failure.
3. Puerperium:
Eclampsia (usually occurs within 48 hour)
Shock (related to reduced sodium and chloride)
Sepsis (due to increased incidence of induction and operative delivery and low vitality).
Remote
1. Residual hypertension: The hypertension may persist even after 6 months following
delivery in about 50% of cases.
2. Recurrent preeclampsia: There is 25% chance of preeclampsia to recur in subsequent
pregnancies.
31.
Preventive Measures
Preeclampsia isnot a very preventable disease. However, some specific 'high risk factors leading to
preeclampsia may be identified in individuals. These are.
1. Primigravida, especially young and elderly.
2. Poor nutrition.
3. Low level of education.
4. Presence of complicating factors like pre-existing hypertension, twins, polyhydramnios, clinical or latent
diabetes and nephritis.
5. History of preeclampsia or hypertension in the family or in previous pregnancy.
6. Abnormal weight gain
.
32.
The following regimeis enforced in such patients in an attempt to prevent or to detect early
manifestations of preeclampsia:
1. Regular antenatal check-up at frequent intervals from t the beginning of pregnancy to detect at the earliest.
The rapid gain in weight or a tendency of rising blood pressure especially the diastolic pressure
2. Advice to take adequate rest in bed on her left side at least for 2 hours in the afternoon from the 20th week
of pregnancy onwards.
3. Low dose aspirin (60 mg) daily, beginning early in pregnancy to potentially high-risk women. It
selectively reduces platelet thromboxane production.
4. Calcium supplementation (2 g/day) reduces the risk of pre-eclampsia
5. Antioxidants, vitamin C and E from 16 to 22 weeks onwards.
Well-balanced diet, which is rich in protein
33.
Management and Nurse'sRole
As the etiology of preeclampsia remains unclear, the management is mostly empirical and symptomatic.
Objectives of care are to:
Provide rest and a tranquil environment
Monitor the condition
Prevent eclampsia and other complications
Deliver a healthy baby in optimal time with minimum maternal morbidity.
a. ECLAMPSIA
Preeclampsia when complicated with convulsion and/or coma is called eclampsia. The term eclampsia is
derived from a Greek word meaning like a flash of lightning It may occur quite abruptly without any warning
manifestations In majority (over 80%), the disease is preceded by features of severe preeclampsia. Thus, it may
occur in women with preeclampsia or in women who have preeclampsia superimposed on essential
hypertension or chronic nephritis
34.
Incidence
The incidence varieswidely from country to country and even between different zones in the same country. In
the developed countries, its prevalence is estimated to be around 1 in 2,000 deliveries. In the developing
countries, particularly in the rural areas, it contributes significantly to the maternal deaths. The hospital
incidence in India ranges from 1 in 500 to 1 in 30. It is more common in primigravida (75%), five times more
common in twins than in singleton pregnancies and occurs between the 36th week and term in more than 50%
(Dutta, 2001).
Pathophysiology
Since eclampsia is a severe form of preeclampsia, the histopathological and biochemical changes are similar
although intensified than those of preeclampsia.
35.
Onset of Convulsions
Convulsionsoccur more frequently beyond 36th week. On rare occasions, convulsion may occur in early months
as in hydatidiform mole:
1. Antepartum (50%): Fits occur before the onset of labour. More often, labour starts soon after and at times, it is
impossible to differentiate it from intrapartum fits.
2. Intrapartum (30%): Fits occur for the first time during labour
3. Postpartum (20 %): Fits occur for the first time in puerperium usually within 48 hours of delivery.
Except on rare occasions, an eclamptic patient always shows previous manifestations of acute fulminating
preeclampsia called premonitory symptoms.
Stage of coma Following the convulsion, the patient passes on to the stage of coma. It may last for a brief period
or may persist until another convulsions. At times, the patient appears to be in a confused state following the fit
and fails to remember the happenings. Rarely coma occurs thout convulsion.
36.
Eclamptic Convulsions
The convulsionsare epileptiform and consist of four stages.
1. Premonitory stage The patient becomes unconscious. There is twitching of the muscles of the face, tongue and
limbs. Eyeballs are rolled or turned to one side and become fixed. This stage lasts for about 30 seconds.
2. Tonic stage The whole body goes into a tonic spasm. The trunk opisthotonus, limbs are fixed and hands
clenched.
3. Clonic stage All the voluntary muscles undergo alternate contractions and relaxation. The twitching’s start in
the face. and then involve one side of the extremities and ultimately the whole body is involved in the
convulsion, Biting of the tongue occurs, breathing becomes stertorous and blood-stained frothy secretions fill
the mouth Cyanosis gradually disappears. This stage lasts for 1-4 minutes.
4. Stage of coma Following the convulsion, the patient passes on to the stage of coma. It may last for a brief
period or may persist until another convulsions. At times, the patient appears to be in a confused state following
the fit and fails to remember the happenings. Rarely coma
37.
Management
The patient, ifat home or in the peripheral health canters, should be shifted urgently
to the referral hospitals. The patient must be heavily sedated before moving her to
the hospital. The aims of immediate management in the hospital are to:
Clear and maintain the airway
Prevent hypoxia
Prevent injury
Arrest convulsions
Effect delivery in 6-8 hours.
The midwife must remain with the mother constantly. In the first instance, all effort
is devoted to the preservation of the mother's life:
38.
1. The patientshould be placed in a railed cot in an isolated room, protected from noxious stimuli,
which might provoke further fits. The patient is to be positioned in semi prone position in order to
facilitate drainage of saliva and vomit. Side lying position helps to minimize vena caval
compression. If the patient is unconscious, the position should be changed at intervals to prevent
hypostatic pneumonia and bedsore. Airway is maintained and oxygen administered to prevent
severe hypoxia
2. Detailed history is to be taken from the relatives relevant to the diagnosis of eclampsia-duration of
pregnancy, number of fits and the medications administered outside.
3. After the patient is properly sedated, thorough, but quick general, abdominal and vaginal
examinations are done. A self-retaining catheter is introduced and the urine is tested for protein.
Continuous drainage is established for measurement of the urinary output. periodic urinary analysis
and for prevention of soiling of the bed due to incontinence likely to occur during p fits.
39.
1. Vital signscheck (pulse, respiration and blood pressure) Is is to be done at every 30
minutes and recorded. Progress of labour and FHR must be monitored. Urinary
output is to be noted hourly,
2. Fluid balance: Crystalloid solution (Ringer's lactate) is A started as a first choice.
Total fluids should not exceed the previous 24 hours urinary output plus 1,000 mL b
(insensible loss through lungs and skin). Normally, it should not exceed 2 L in 24
hours. In preeclampsia and eclampsia, although there is hypovolemia, the tissues 10
are overloaded.
3. Anticonvulsant therapy is given to control the fit and to prevent its recurrence.
Magnesium sulfate is the A drug of choice. It reduces motor end-plate sensitivity to
acetylcholine and thereby reduces neuromuscular irritability. Magnesium sulfate
induces cerebral vasodilation, dilates uterine arteries and inhibits platelet activation.
It has no detrimental effects on the R neonate within therapeutic level.
40.
Administration of magnesiumsulfate
The regimens given below may vary between hospitals:
1. Pritchard regimen:
Loading dose: 4 g IV over 3-4 minutes (20 mL of 20% solution) and then 10 g deep intramuscular (IM)
Maintenance dose: 5 g IM in alternate buttock 4 hourly (10 mL of 50% solution).
1. Zuspan regimen:
Loading dose: 4 g IV over 5-10 minutes
Maintenance dose: 2 g/h IV infusion.
1. Sibai regimen:
Loading dose: 6 g IV over 20 minutes
Antihypertensive and diuretics
In spite of anticonvulsant and sedative regimen, if blood pressure remains more than 160/110 mm Hg.
antihypertensive drugs are administered. Hydralazine 5 mg IV is given slowly and repeated after 20 minutes with 10
mg, if there is no response. The blood pressure should be monitored at every 5 minutes. Hydralazine is repeated
whenever the diastolic pressure rises to 110 mm Hg. Alternatively, labetalol is given by slow IV route 20 mg/h for
smooth control of blood pressure. Presence of pulmonary oedema requires diuretics. In such cases, furosemide is
administered in doses of 20-40 mg intravenously and repeated at intervals.
41.
Role of themidwife
1. The woman should be placed in a sound protected room to minimize auditory stimulation.
2. Eye pads to be applied to minimize optic stimulation
3. The room should be well-lighted so as not to miss the development of cyanosis.
4. Bed railings to be padded in order to minimize physical injury during convulsion.
5. Patient to be placed in semi prone position and the position to be changed at every 2 hours, if the
patient is heavily sedated or in deep coma to avoid hypostatic pneumonia and bedsores.
6. Keep Foley's catheter in the urinary bladder and make chart of urinary output every hour.
7. Minimal handling and stimulation in order to reduce the risk of occurrence of another convulsion.
8. Maintain an IV line patent preferably in a central vein.
9. Keep a tracheotomy tray available
10. Apply a thromboelastic stocking to prevent deep vein thrombosis.
42.
Management during afit
1. In the premonitory state, a mouth gag is to be placed in between the teeth to prevent tongue bite and should be
removed after the Clonic phase is over.
2. The air passage is to be cleared off the mucus with a mucus sucker after convulsion.
3. The patient's head is to be turned to one side and the pillow taken off. Raising the foot end of the bed
facilitates postural drainage of the upper respiratory tract
4. Oxygen is to be given until cyanosis subsides. The parameters to monitor are-a return to normal blood
pressure, an increase in urinary output, a reduction in oedema and a return to normal laboratory indices.
Complications of Eclampsia
Injuries: Tongue bite, injuries due to falling out of bed
Cardiovascular: Vasospasm, pulmonary embolism
Renal: Oliguria, renal failure
Haematological: Hypovolemia, hemoconcentration, thrombocytopenia, DIC
Neurological: Cerebral oedema, cerebral hemorrhage Hepatic; Subcapsular hematoma, hepatic necrosis
Respiratory: Pneumonia (aspiration, hypostatic or infective)
Sensory: Disturbed vision due to retinal oedema or detachment (usually reversible) Puerperal: Sepsis,
psychosis
Fetal: Placental abruption, intrauterine growth retardation, fetal distress, intrauterine death.
43.
OBSTETRIC SHOCK
Shock isdefined as a state of circulatory inadequacy with poor tissue perfusion resulting in generalized cellular
hypoxia leading to dysfunction of organs and cells.
Shock can be acute, but prompt treatment results in recovery with little detrimental effect on the mother.
However, inadequate treatment or failure to initiate effective treatment can result in chronic multisystem organ
failure, which may be fatal.
44.
1. Neurogenic shock:
a.Chemical Injury: Associated with aspiration of gastrointestinal contents during
general anesthesia, especially in cesarean section (Mendelson's syndrome).
b. Drug induced: Associated with spinal anesthesia.
2. Shock (endotoxic shock): Typically associated with septic abortion,
chorioamnionitis, pyelonephritis and rarely postpartum endometritis. This type of
shock may be hypovolemic, but has primary cardiogenic and cellular components
also. In this section, hypovolemic shock and septic shock are discussed as either of
which may occur because of childbearing,
45.
Stages of shock
Thebody reacts to the loss of circulating fluid in stages as follows:
1. Initial stage: The reduction in fluid or blood decreases the venous return to the heart. The ventricles of the
heart are inadequately filled, causing a reduction in stroke volume and cardiac output. As cardiac output and
venous return fall, the blood pressure is reduced. The drop in blood pressure decreases the supply of oxygen to
the tissues and cell function is affected.
2. Compensatory stage: The drop in cardiac output produces a response from the sympathetic nervous system
through the activation of receptors in the aorta and carotid arteries. Blood is redistributed to the vital organs.
Vessels in the gastrointestinal tract, kidneys, skin and lungs constrict. The response is seen by the skin
becoming pale and cool. Peristalsis slows, urinary output is reduced and exchange of gas in the lungs is
impaired. The heart rate increases in an attempt to improve cardiac output and blood pressure. Pupils of the
eyes dilate. The sweat glands are stimulated and the skin become moist and clammy.
46.
Adrenaline and aldosteronefrom adrenal gland and anti-diuretic hormone from posterior gland are screated
causing vasoconstriction, an Increased cardiac output are and a decrease in urinary output Venous to the heart
will increase but unless the fund less is replaced, this will not be sustained
3 . Progressive stage : This stage leads to multisystem failure Compensatory mechanisms begin to fall with vital
organs lacking adequate perfusion. Volume depletion causes further fall in blood pressure and cardiac output. The
coronary arteries suffer lack of supply Peripheral circulation is poor, with weak or absent pulses
1. Late stage (irreversible) Hypotension continues and cannot be reversed by replacement
of fluid because of stagnation of blood at the microvascular level. Colour of skin becomes ashen gray
Metabolic acidosis starts and for elimination of accumulated carbon dioxide. the respiratory rate becomes
rapid. Imperceptible low volume pulse, oliguria and mental confusion occur Multisystem failure and cell
destruction are irreparable. Treatment of any kind is practically useless in this phase, Death ensues (Dutta,
2001).
47.
Management
Urgent resuscitation isneeded to prevent the mother's condition from deteriorating and causing irreversible
damage. The priorities are tog
1. Maintain the airway: If the mother is severely collapsed, she should be turned on to her side and oxygen
administered at a rate of 6-8 L/min. If she is unconscious, endotracheal intubation may be necessary.
2. Replace fluids (infusion and transfusion) Blood should be taken for cross matching prior to
commencing intravenous fluids. A plasma expander or fresh frozen plasma is given until whole blood is
anav
3. Avoid warmth Constriction of the peripheral blood supply occurs in response to the shock keeping the
mother warm may interfere with this response. causing further deterioration in her condition
4 .Control of hemorrhage Specific surgical and medical treatment for control of hemorrhage should start
along with the general management of shock
48.
Clinical observations forthe mother in shock (Monitoring)
Assess the level of consciousness, signs of restlessness and confusion are to be noted blood
Monitor blood pressure every 30 minutes or continuously
The cardiac rhythm may be monitored continuously
Assess skin colour and temperature hourly
Assess central venous pressure and fluid balance for adequacy of circulating volume
Watch for occurrence of any further bleeding.
49.
Clinical signs
1. Inthe initial phase, there is marked flushing of the and the skin feels war
2. Temperature rise varies from 101°F to 105°F
3. Tachycardia, tachypnea and rigors occur.
Hemorrhage may be present, which either could be due to the events of childbearing or because of disseminated
intravascular coagulation.
5. As vasodilatation continues, hypotension leads to kidney damage with reduced glomerular filtration and acute
tubular necrosis and oliguria.
6. If the shock condition does not improve, the patient passes clinically to the stage of irreversible shock. She
remains cold and clammy with ashen gray cyanotic appearance.
7. Anuria, cardiac or respiratory distress and coma may supervene.
8. Disseminated intravascular coagulation is also a feature of septic shock
9. Multisystem organ failure will result as an effect of the continued hypotension and myocardial depression.
Failure of the liver, brain and respiratory systems follows, and death results.
50.
Management
Management is basedon preventing further deterioration by restoring circulatory volume and eradication of the
infection. A full infection screening should be carried out including a high vaginal swab, midstream urine and blood
cultures, Retained products of conception if detected on ultrasound should be removed.
Measures of management include Intravenous administration of antibiotics, intravenous fluids, adjustment of acid-
base balance, steroids, prevention and treatment of intravascular coagulation and toxic myocarditis, administration
of oxygen and elimination of the source of infection. These are as follows:
1. Antibiotics: Broad-spectrum antibiotics are given to start with and after confirming the sensitivity, specific
antibiotics are given intravenously.
2. Intravenous fluids and electrolytes: Septic shock associated haemorrhagic hypotension is treated with liberal
infusion and blood transfusion. Oliguria with high specific gravity is an indication for liberal fluid administration,
whereas a low specific gravity indicates fluid restriction. Impairment of renal function contraindicates
administration of electrolytes.
51.
. Correction ofacidosis: Bicarbonate is administered to correct metabolic acidosis.
4. Maintenance of blood pressure: Inotropic agents such as adrenaline, noradrenaline, dopamine and
dobutamine are administered to increase the cardiac contractility. Vasodilator drugs such as sodium
nitroprusside, nitroglycerin and diuretics are used in selected cases to reduce the after load and pulmonary
oedema.
5. Corticosteroids are given to exert an antiendotoxin effect and to counteract anaerobic oxidative mechanism.
6. As a prophylactic measure for DIC, heparin may be given. Fresh frozen plasma or whole blood transfusion
may be used.
7. In unresponsive septic shock following septic abortion or puerperal sepsis, hysterectomy may be done to
eliminate the source of infection.
The mother may require care and management in a critical or intensive care unit. The family should be kept
informed of progress.
52.
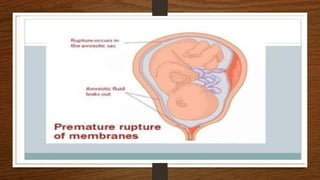
a. PREMATURE RUPTUREOF MEMBRANE
OPROM is define as...."Rupture of membrane Or Breakage of Amniotic sac" More than
1 hour before the onset of labour
OPROM is define as...."Rupture of membrane Or Breakage of Amniotic sac" More than
1 hour before the onset of labour preterm
Premature rupture of membranes - In this type of PROM membrane that
rupture...."Before the 37 week of gestational age"
Prolonged premature rupture of membranes - In this type of rupture....."24 hours has
passed between membrane rupture And onset of labour"
Previable preterm Previable preterm rupture of membranes - This type of rupture
occurs..."Before 24 weeks of gestational age of fetus" (It is also known as mid-trimester
PPROM)
54.
Cause
Weakening ofmembranes
Constructed uterus
Extreme force of contraction of uterus
Risk Factors
Infection
UTI
STDs
Bacterial vaginosis o Amniotic Sac infection
Smoking during pregnancy
Previous history of PROM Previous history of Preterm
Hemorrhage or bleeding any time
Polyhydramnios
Multiple pregnancy
Sign and symptoms
Painless leakage of fluid from vagina.
Due to loss of fluid fetal can easily feel through
belly.
Decrease uterine size
Meconium present in fluid
Abdominal pain
Fetal heart sound altered
Gush of membrane
Absence of steady labour contraction
Diagnostic Evaluation
History collection of
Previous labour Maternal history
Maternal illness
Fetal movement assessment
Fetal position
Blood analysis
Sterile speculum examination (to assess the inside of
vagina)
55.
Treatment
Treatment depends onthe number of weeks of pregnancy at which this happens. If PROM occurs before 37
weeks the mother is given intravenous antibiotics. If the baby is close to term, the mother is usually advised to
have her labour induced. Induction of labour is not always needed if contractions start within 24 hours of rupture
(unless the mother
Nursing
Hospitalization of woman
Evaluated for labour
Fetal distress
Infection
Complete bed rest
Continuous observe the fetal movements
Continuous assess the vital signs of mother has had a test during the pregnancy that is positive for a bug called
GBS that can make babies very unwell).
56.
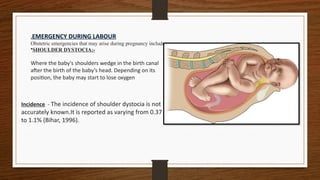
.EMERGENCY DURING LABOUR
Obstetricemergencies that may arise during pregnancy include
•SHOULDER DYSTOCIA:-
Where the baby's shoulders wedge in the birth canal
after the birth of the baby’s head. Depending on its
position, the baby may start to lose oxygen
Incidence - The incidence of shoulder dystocia is not
accurately known.It is reported as varying from 0.37
to 1.1% (Bihar, 1996).
57.
Risk Factors
The possibilityof shoulder dystocia should be anticipated anytime when any of the following conditions exist:
Maternal diabetes
Obstetric history of large babies (over 4,000 g)
Family history of large siblings Maternal obesity (over 90 kg)
Large fetus (fetal macrosomia, over 4,000 g)
Any estimated fetal weight 500 g or more greater than the woman's largest previous baby
Maternal age over 35 years
High parity.
58.
Warning Signs andDiagnosis
The delivery of the head with or without forceps may have ge been quite easy, but more commonly the
head may have advanced slowly and the chin may have had difficulty sweeping over the perineum. Once
the head is delivered, it may look as if it is trying to return to the vagina. It is caused by shoulder traction
and is called the turtle sign.
Shoulder dystocia is diagnosed when the manoeuvres normally used by the midwife fails to accomplish
delivery (Resnik, 1980). It is important for the midwife to know how to manage this situation because, even
with anticipation, diagnosis cannot be made until after the head is born. This the gives little time to resolve
the problem before the baby is either damaged or dead.
62.
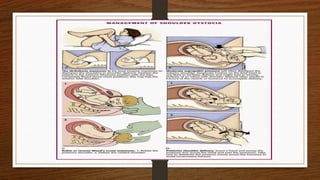
Management
The following stepsshould be taken in sequence to manage the the emergency of shoulder dystocia:
Stay calm and ensure mother's cooperation
Request that an obstetrician, an anaesthetist neonatologist be called stat
Request readiness of a full-scale new-borns resuscitation efforts
Request readiness to manage an immediate postpartum hemorrhage
The obstetrician may try the following manoeuvres to dislodge the shoulders and deliver the baby:
1) Check position of the shoulders and rotate them into one of the oblique diameters of the pelvis. Instruct the
mother not to push. Rotation is accomplished by placing all the fingers of one hand on one side of the baby's
chest, and all the fingers of the other hand on the baby's back on the opposite side and pressing with the
amount of force necessary to move the baby
2) It is necessary that the entire hand is used and not just two fingers for maximum strength. Under no
circumstances, the baby's head should be moved as this would result in injury to the brachial or cervical nerve
plexus or fracture of the cervical vertebrae.
63.
.
1) Downward andoutward pressure is applied on the sides of the baby's head, while another person applies
suprapubic pressure.
Suprapubic pressure is most effective if the person applying it stands on a footstool in order to get greater force
behind the downward push. In mild dystocia, the baby may be delivered with this step.
Under no circumstances, allow the fundal pressure to be applied erroneously. This will only further impact
shoulders, waste time, possibly cause injury to the fetus and possibly rupture the uterus with disastrous sequelae
to both mother and baby.
1) The baby is not delivered
Cut or enlarge the episiotomy. A deep mediolateral episiotomy will allow more room for manipulation.
Catheterize the woman to empty her bladder.
Place the woman in an exaggerated lithotomy.
Do a vaginal examination to rule out causes of shoulder dystocia (after the head is born) other than impacted
shoulders. This requires the insertion of the entire hand as far as it can be in. Other causes to be ruled out at
this stage are:
64.
1) The babyis not delivered
Cut or enlarge the episiotomy. A deep mediolateral episiotomy will allow more room
for manipulation.
Catheterize the woman to empty her bladder.
Place the woman in an exaggerated lithotomy.
Do a vaginal examination to rule out causes of shoulder dystocia (after the head is
born) other than impacted shoulders. This requires the insertion of the entire hand as
far as it can be in. Other causes to be ruled out at this stage are:
Short umbilical cord (relative or absolute)
Enlargement of the thorax or omen of the fetus might be caused by tumour’s or severe
oedema
Conjoined twins
Bandls retraction ring.
If the dystocia is diagnosed as resulting from shoulder dystocia, attempt is made again
to deliver the baby by the application of suprapubic pressure, while the obstetrician
uses firm downward and outward pressure on the side of the baby's head. The baby
Rupture of t may be delivered after this step if the condition was a moderate shoulder
dystocia.
Maternal
The maternal riskare incidental due to emergency operative delivery, which
involves the risk of anaesthesia, blood loss and infection
Fetal
The fetus is at risk of anoxia due to acute placental insufficiency from the moment
cord is prolapsed. The blood flow is occluded either due to mechanical compression
by the presenting part against the incompletely dilated cervix/pelvic wall or due to
vasospasm of the umbilical vessels due to exposure to cold or irritation, when
exposed outside the vulva or as a result of handling. The danger is more in vertex
presentation, especially when the prolapse is through the anterior segment of the
pelvis or when the cervix is partially dilated.
71.
Management of CordProlapse
Immediate Action
1) When diagnosis of cord prolapse is made, the midwife calls for urgent assistance.
2) The mother and her family must be given explanation about the findings and the emergency measures that
will be needed.
3) If oxytocin infusion is in progress, it should be stopped.
4) If the baby is alive, the aim of immediate management is to minimize pressure on the cord until such time
when the woman is prepared for assisted delivery or is transferred to an equipped hospital. For this, the
gloved fingers are to be introduced into the vagina to lift the presenting part of the cord. The fingers should
be placed inside the vagina until definitive treatment is instituted
5) Postural treatment is given until the delivery of the baby, either vaginally or by cesarean section. The
woman is placed in exaggerated elevated Sims' position. with pillow under the hip. The foot end of the bed
may be elevated. High Trendelenburg or knee-chest position, which has been traditionally mentioned, is
very tiring and distressing to the woman.
6) If much cord lies outside the vagina, it should be replaced into the vagina to minimize vasospasm due to
irritation and to maintain the temperature.
7) If much of the cord is outside the vulva, it should be covered with sterile wet gauze, to prevent spasm of the
umbilical vessels due to draughts.
72.
Definitive Management
1. Cesareansection is the ideal management when the baby is sufficiently mature enough
to survive. Where the fetus is confirmed alive and delivery is not imminent, the birth must
be expedited with the greatest possible speed to reduce the mortality and morbidity
associated with this condition.
2. If immediate cesarean section is not possible or the baby is too premature, reposition of
the cord may be an alternative. The cervix must be at least half dilated and the cord
wrapped in a large piece of sterile roller gauze, is manually pushed above the presenting
part under general anaesthesia. This is followed by stimulation of uterine contraction with
oxytocin drip, if necessary. When the cervix is about three-fourth dilated, ventouse traction
may be applied to deliver the baby. This is possible only with vertex presentation and
carries high fetal risks.
3. If the head is engaged, delivery is completed by forceps. With a breech engaged, a
breech extraction is done. 4. If the fetus is confirmed dead, labor is allowed to proceed,
awaiting spontaneous termination.
73.
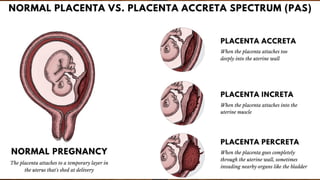
a. PLACENTAACCRETA –
Placentaaccreta is an abnormal partial or total adherence of the placenta to the uterine wall. The placenta is
directly adhered to the myometrium with either defective decidua or no decidua in between. When the chorionic
villi extent Inversion further than contact with the myometrium and actually threate penetrate the uterine wall,
the condition is called placenta out par increta. Placenta percreta occurs when the chorionic villi invade through
the entire uterine wall to the serosa layer. These conditions are rare complications.
The probable cause is defective decidual formation. The condition is usually associated with placenta previa. It
may also occur when the placenta is situated over injured sites as following cesarean section, dilation and
curettage operation, manual removal or myomectomy.
75.
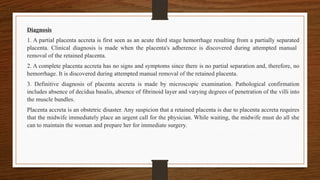
Diagnosis
1. A partialplacenta accreta is first seen as an acute third stage hemorrhage resulting from a partially separated
placenta. Clinical diagnosis is made when the placenta's adherence is discovered during attempted manual
removal of the retained placenta.
2. A complete placenta accreta has no signs and symptoms since there is no partial separation and, therefore, no
hemorrhage. It is discovered during attempted manual removal of the retained placenta.
3. Definitive diagnosis of placenta accreta is made by microscopic examination. Pathological confirmation
includes absence of decidua basalis, absence of fibrinoid layer and varying degrees of penetration of the villi into
the muscle bundles.
Placenta accreta is an obstetric disaster. Any suspicion that a retained placenta is due to placenta accreta requires
that the midwife immediately place an urgent call for the physician. While waiting, the midwife must do all she
can to maintain the woman and prepare her for immediate surgery.
76.
Management
1. In partialplacenta accreta, where major separation is possible, the adherent area is separated manually
leaving behind bits of placental tissue with the uterine wall. Oxytocin is administered for uterine contraction
and intrauterine plugging to achieve homeostasis. If the uterus fails to contract, hysterectomy is done.
2. In complete placenta accreta, hysterectomy is done in parous women. In women desiring to have another
child, conservative management may be undertaken. This consists of cutting the umbilical cord as high as
possible and leaving behind the placenta, which is expected to be autolyzed in due course of time. Appropriate
antibiotics are given. Risk of placenta accreta include hemorrhage, shock, infection and rarely Inversion of
uterus.
77.
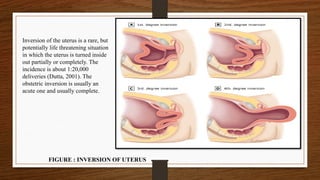
Inversion of theuterus is a rare, but
potentially life threatening situation
in which the uterus is turned inside
out partially or completely. The
incidence is about 1:20,000
deliveries (Dutta, 2001). The
obstetric inversion is usually an
acute one and usually complete.
FIGURE : INVERSION OF UTERUS
78.
Classification of Inversion
1)First degree: There is dimpling of the fundus, which remains above the level of the internal os.
2) Second degree: The uterus is inverted and the fundus passes through the cervix, but lies inside the vagina.
3) Third degree (complete): The endometrium with or without the attached placenta is visible outside the vulva.
The uterus, cervix and part of the vagina are inverted and visible.
Causes
The inversion may be spontaneous or more commonly induced.
Spontaneous (40%)
Spontaneous is brought about by local atony of the placental site over the fundus associated with sharp rise of
intra-abdominal pressure as in coughing, sneezing or bearing down effort. Fundal attachment of the placenta,
short cord and placenta accreta are often associated.
.
79.
.
.
Presentation
Uterine inversion maypresent:
Acutely-within 24 hours of delivery
Sub acutely-over 24 hours and up to 30th postpartum day
Chronic-more than 30 days after delivery.
It presents most often with classic symptoms of postpartum hemorrhage
Sudden appearance of a vaginal mass
Cardiovascular collapse of varying degree.
Induced (60%)
Induced is due to mismanagement of third stage of labour:
Pulling the cord when the uterus is atonic specially when combined with fundal pressure
Crede's method of placental expression, while the uterus is relaxed
Faulty technique in manual removal: Pulling the partially separated placenta, or firmly pressing on the atonic
uterus by the external hand or rapidly withdrawing the internal hand thereby creating a negative pressure.
80.
Danger
Shock, whichis profound and mainly neurogenic in origin due to:
Tension on the nerves from stretching of the infundibulo pelvic ligament
Pressure on the ovaries as they are dragged with the fundus
Peritoneal irritation.
Hemorrhage, especially after detachment of placenta
Pulmonary embolism
Infection and uterine sloughing, if left uncared.
Induced is due to mismanagement of third stage of uncare : Pulling the cord when the uterus is atonic specially
when
combined with fundal pressure : Crede's method of placental expression, while the uterus is relaxed Faulty
technique in manual removal: Pulling the partially separated placenta, or firmly pressing on the atonic uterus by
the external hand or rapidly withdrawing the internal hand thereby creating a negative pressure.
81.
Diagnosis
Acute lowerabdominal pain with bearing down sensation
Varying degree of shock
On abdominal examination:
Dimpling or cupping of the fundal surface
Fundus cannot be palpated.
Incomplete variety, a pear-shaped mass protrudes outside the vulva with the broad end pointing
downwards and looking reddish purple in colour
82.
Management
Before Shock Develops
Immediatemedical support must be summoned. Urgent manual replacement (even without anaesthesia if
not easily available) must be done as outlined below
1) To push the fundus with the palm of the hand, along the direction of the vagina toward the posterior fornix
2) To apply counter support with the other hand placed the abdomen
3) After replacement, the hand should remain inside the uterus until the uterus becomes contracted by
parenteral oxytocics
4) The placenta is to be removed manually only after the uterus becomes contracted; a partially separated
placenta may be removed prior to replacement to reduce the bulk, which facilitates replacement.
5) Usual treatment of shock including blood transfusion should be arranged as and when required.
83.
Avoid pullingthe cord simultaneous with fundal pressure.
Prevention
Do not employ any method to expel the placenta out when the uterus is relaxed
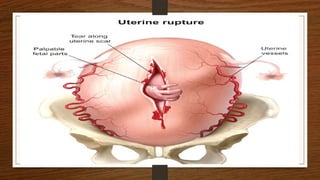
a. RUPTURE OF UTERUS - complete rupture when it involves a tear in the wall of the uterus including
the peritoneal coat and with or without expulsion of the fetus. Incomplete rupture is tearing of the uterine
wall without involving the perimetrium. Life of both mother and fetus may be endangered in either
situation.
After Shock Develops
1) The treatment of shock should be instituted vigorously. Morphine 15 mg
intramuscularly, dextrose saline drip and arrangements for blood transfusion to be
made.
2) To push the uterus inside the vagina if possible and to pack the vagina with
antiseptic roller gauze.
3) Foot end of the bed to be raised.
4) Replacement of the uterus under general anaesthesia to be done along with
resuscitative measures.
85.
Rupture of theUterus
Spontaneous rupture of the uterus can be precipitated in the following circumstance
High parity
Injudicious use of oxytocin, particularly where the mother is of high parity
Obstructed labour: The uterus ruptures due to excessive thinning of the lower sparity
Neglected labour, where there is previous history of cesarean section Extension of cervical laceration upwards
into the lower uterine segment
Trauma as a result of accident or injury Perforation of a non-pregnant uterus may result in rupture in a
subsequent pregnancy, usually in the upper uterine segment
a. Antenatal rupture of the uterus may occur where there has been a history of previous classical cesarean
section.
A break in the continuity of the uterine wall any time beyond 28 weeks of pregnancy is called rupture of the uterus. The rupture
is described as
86.
Signs of IntrapartumRupture of the Uterus
A complete rupture of a non-scarred uterus may be accompanied by:
Sudden collapse of the mother who complains of severe abdominal pain
Increase of maternal pulse rate
Alteration of fetal heart rate including the presence of variable decelerations on the monitor strip Fresh
vaginal bleeding
Uterine contractions may stop and the contour of abdomen alters
Fetal heart sounds may be lost
fetus becomes palpable in the abdomen as the presenting part regresses
The mother goes into shock, the degree of which depends on the extent of the rupture and the blood loss.
.
87.
Signs of IncompleteRupture
rupture may have an insidious onset or
may be silent and usually discovered
after delivery or during a cesarean
section. This is more commonly
associated with ebrais previous
cesarean section.
Blood loss associated with incomplete
rupture can be scanty as the rupture
occurs along the fibrous scar tissue.
Incomplete rupture may also manifest
as postpartum hemorrhage following
vaginal delivery. Whenever shock
during third stage is more severe than
the blood loss warrants or the mother
fails to respond to treatment given, the
possibility of incomplete rupture
should be considered.
88.
Management
Depending upon thestate of the clinical condition, resuscitation needs to be done followed by laparotomy,
or in acute conditions; resuscitation and laparotomy are to be done simultaneously. Following laparotomy
any of the following procedures may be adopted:
Hysterectomy in spontaneous obstructive rupture; a quick subtotal hysterectomy is usually done Repair is
mostly applicable in cases of scar rupture where the margins are clean
Repair and sterilization (tubal ligation) is mostly done in patients with a clean cut scar rupture having
desired number of children.
The mother will be unprepared for the events that have occurred and therefore may be totally opposed to
hysterectomy. Explanation and preparation of both mother and family are important though this is an
emergency situation.
89.
a. AMNIOTIC FLUIDEMBOLISM –
An amniotic fluid embolism is rare but serious condition that occur when amniotic fluid, fetal material, such as
hair, enters the maternal bloodstream.
The body respond in 2 phases
The initial phase is one of pulmonary vasospasm causing hypoxia, hypotension, pulmonary oedema and
cardiovascular collapse.
The second phase sees the development of left ventricular failure, with haemorrhage and coagulation
disorders and further uncontrollable haemorrhage
Etiology
A maternal age of 35 years
older Caesarean or instrumental vaginal delivery
Polyhydramnios Cervical laceration or uterine rupture o Placenta previa or abruption
Amniocentesis o Eclampsia
Abdominal trauma
Ruptured uterine or cervical veins.
Ruptured membranes
91.
Sign and symptoms
Sudden shortness of breath o Excess fluid in the lungs
Sudden low blood pressure
Sudden circulatory failure Life threatening problems with blood clotting
(disseminated intravascular coagulopathy)
Altered mental status o Nausea or vomiting
Chills
Rapid heart rate
Fetal distress
Seizures
Coma
Management
Maintain systolic blood pressure > 90 mmHg.
Urine output > 25 ml/hr
Re-establishing uterine tone
Correct coagulation abnormalities o Administer oxygen to maintain normal saturation. o
Intubate if necessary.
Initiate cardiopulmonary resuscitation (CPR) if the patient arrests. If she does not respond
to resuscitation, perform a cesarean delivery
92.
.
Treat hypotensionwith crystalloid and blood prodeliver
Consider pulmonary artery catheterization in patients who are haemodynamically unstable.
Continuously monitor the fetus.
trauma to the uterus must be avoided during manoeuvres such as insertion of a pressure catheter or rupture of
membranes.
Incision of the placenta during caesarean delivery should also be avoided
Incision of the placenta during caesarean delivery should also be avoided
Nursing management
Give immediate and vigorous treatment.
Give oxygen by face mask.
Maintain normal blood volume through administration of plasma and intravenous fluids.
Prevent development of disseminated intravascular coagulation (DIC). Serious complications can occur.
Administer whole blood and fibrinogen.
Monitor the patient's vital signs. o Deliver the fetus as soon as possible
93.
Etiology
This meansthe baby will not grow and a miscarriage occurs.
Sometimes, often for unknown reasons, a miscarriage may occur many weeks into a seemingly healthy
pregnancy.
Other obstetric emergencies can be caused by a number of factors, such as trauma or for genetic reasons.
Sometimes a woman’s experience in earlier pregnancies can help her doctor identify possible
complications and prepare for tsib cut
Any bleeding during pregnancy is not normal – be sure to call your doctor or midwife
Heavy bleeding with severe stomach pain in the first three months of pregnancy – could be a sign of
ectopic pregnancy
Heavy bleeding with cramping in the first three to four months of pregnancy – could be a sign of
miscarriage
Bleeding with abdominal pain in the last three months of pregnancy – could be a sign of placental
abruption
An early pregnancy complication usually occurs because the developing baby has not properly attached or formed.
94.
Stomach cramps– could be a sign of ectopic pregnancy
Dizziness – could be a sign of ectopic pregnancy or pre-eclampsia
Severe vomiting or sickness – could be a severe symptom of pregnancy, or could be due to an infection
Severe stomach pain – could be a sign of pre-eclampsia
Lower back pain – could be a sign of pre-eclampsia
Rapid increase in blood pressure, possibly signalled by nose bleeds, headache or dizziness could be a sign of
pre-eclampsia
• Blurry vision and headaches – could be a sign of pre-eclampsia
• Sudden and significant swelling of hands, face and feet – could be a sign of pre-eclampsia
• Fever – could be a sign of an infection
• A decrease in your baby’s normal daily movements, or if you are worried about how frequently your baby
moves
• Regular, increasingly intense contractions before 37 weeks of pregnancy – might be a sign of premature
labour
• If your waters break before labour begins – you may feel a gush or continual trickle of fluid that has a slightly
sweet smell
95.
. EMERGENCIES DURINGPOSTNATAL PERIOD
PUERPERAL SEPSIS
Puerperal infection is an infection of the genital tract which occurs as a complication of delivery is termed as
Puerperal sepsis /Puerperal infection
Causative organism
Doderlein bacillus (60-70%)
Endometritis
Endomyometritis
Endoparametritis
Yeast like fungus - Candida
Sign and symptoms
Local infection
slight raise in temperature, generalised malaise and headache.
Redness and the swelling of the local wound
Pus formation and disruption of wound
Uterine infection (Mild)
Pyrexia of variable degree and tachycardia.
Red, copius and offensive lochia.
Convoluted, tender and soft uterus.
Uterine infection (Severe infection) • Fever with chills and rigor Rapid pulse
Scanty, odourless lochia
subinvoluted uterus
98.
Intranatal
Staffattending on labour client should be free of infections.
Full surgical asepsis to be taken while conducting delivery
Women having respiratory tract infection or skin infection should be admitted in single room or separate
ward
Membranes should be kept intact as long as possible and vaginal examination should be restricted to
minimum
Antibiotics
Ideal antibiotics regime should depend on the culture and sensitivity report.
Gentamycin 2mg/kg IV loading dosed followed by 1.5 mg/kg IV Q8H and Amphicllin 1gm IV Q6H or
Clindamycin 900mg IV Q8H should be started
Or IV Cefixime 1gm Q8H
99.
Investigation
Complete blood count
Ultrasound(For diagnosis of pelvic mass)
Pelvic abscess
Pelvic peritonitis
Retained bits of placenta and/ or membrane
Other specific investigation
X-ray
Blood for malaria parasite
Prophylaxis during Antenatal
Improvement of general condition
Treatment of septic cocci
Abstinence from sexual intercourse in the last two months
Care about personal hygiene - bathing in dirty water to be avoided
Avoiding contact with people having infection, such as cold, boils.
Avoiding unnecessary vaginal examinations and douches in the later months.
100.
Surgical treatment
There isa very little role of major surgery in the treatment of puerperal sepsis
Puerperal wound
The stitches of the perineal wound may have to be removed to facilitate drainage of pus and relieve
pain.
Metronidazole 0.5 IV Q8H to control anaerobic group Treatment should be for 7-10 days
Retained uterine product
With a diameter of 3cm or less may be disregarded and left alone. Otherwise surgical evacuation after
antibiotic coverage for 24hrs should be done to avoid the risk of septicaemia.
101.
CONCLUSION
Obstetric emergencies wereresponsible for 70.6% of the maternal mortality and 86% of the perinatal
mortality within the period. Conclusion. Prevention/effective management of obstetric emergencies will
help to reduce maternal and perinatal mortality in our environment .























![maternal guide presentation [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/maternalpresentationautosaved-250208125838-a01bbc1b-thumbnail.jpg?width=640&height=640&fit=bounds)
































![managementofnursingeducationalinstitutions-200922164146[2].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/managementofnursingeducationalinstitutions-2009221641462-250314161750-edac83bc-thumbnail.jpg?width=640&height=640&fit=bounds)



















