Downloaded 152 times

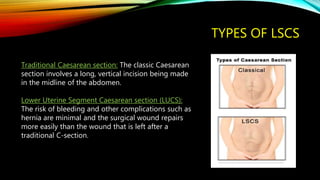
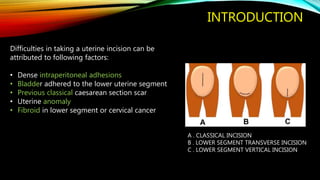






The document provides an extensive overview of the challenges and techniques associated with lower segment caesarean sections (LSCS), including types, indications, and complications. It emphasizes the importance of skilled techniques to manage difficulties such as dense adhesions, bladder injuries, and adherence of the lower uterine segment, and outlines strategies for safe delivery. The conclusion stresses the need for obstetricians to be well-prepared to reduce maternal and fetal morbidity as LSCS rates increase.























































































