PRE-ECLAMPSIA - CASE PRESENTATION: WITH OBSTETRIC EMERGENCIES
This is a case presentation on Obstetric emergencies focusing on pre eclampsia. It introduces Obstetric emergencies , then goes a head to discuss a case on pre eclampsia. Hope learners and professionals likewise benefit from the same.
Introduction
- Many pregnantwomen first present to outpatient clinics with
symptoms that may indicate a life-threatening condition.
- we are often the first line of defense against maternal mortality.
Our role includes:
- Recognizing red flags
- Initiating basic emergency care
- Arranging prompt referrals to higher-level facilities
Our Goal Today:
- Understand the most common obstetric emergencies seen in
outpatient settings
- Learn how to identify them early
- Know what to do before transferring the patient
- Emphasize when and where to refer
3.
Maternal Mortality
Kenya’s Burden:
-According to KDHS 2022: ~358 maternal deaths per 100,000 live births
Majority occur due to delays in:
- Seeking care
- Reaching appropriate care
- Receiving timely & quality care
Outpatient Clinics Are Critical in the Chain of Care
- We can reduce these delays by recognizing danger signs early.
4.
Common Obstetric EmergenciesSeen in Outpatient Clinics
We will focus on these conditions today:
1. Antepartum Hemorrhage (Placenta Previa, Placental Abruption)
2. Hypertensive Disorders of Pregnancy (Preeclampsia, Eclampsia)
3. Postpartum Hemorrhage (PPH)
4. Preterm Labour / Premature Rupture of Membranes (PROM)
5. Puerperal Sepsis
6. Fetal Distress / Decreased Fetal Movements
> Note: Obstructed labor and uterine rupture may not commonly present
here unless referred from home delivery attempts.
5.
1. Antepartum Hemorrhage(APH)
Definition: Vaginal bleeding after 20 weeks gestation but before delivery.
Common Causes:
- Placenta Previa: Painless bleeding, low-lying placenta
- Placental Abruption: Painful bleeding, tender uterus, associated with HTN or trauma
What You Can Do:
- Take a detailed history
- Avoid vaginal exams if previa suspected
- Check BP, pulse, fetal movements
- Start IV fluids if needed
- Arrange urgent referral to hospital
6.
2. Hypertensive Disordersin Pregnancy
Includes:
- Gestational Hypertension
- Preeclampsia
- Eclampsia
Red Flags:
- BP ≥140/90 mmHg + proteinuria or other organ dysfunction
- Headache, visual disturbances, epigastric pain
- Swelling of face/hands
- Seizures (Eclampsia)
Immediate Actions:
- Measure BP urgently
- Administer magnesium sulfate for seizure prevention/treatment
- Use labetalol or hydralazine to control severe hypertension
- Refer immediately for delivery
7.
3. Postpartum Hemorrhage(PPH)
Definition: Blood loss ≥500ml after vaginal delivery or ≥1000ml after C-section.
Most Common Cause: Uterine atony
The 4Ts of PPH- Tone, Thrombocytopenia, Tissue, Trauma
Symptoms to Watch For:
- Excessive bleeding after delivery
- Clots >5cm
- Unresponsive fundus
- Signs of shock (tachycardia, hypotension)
In our Setting:
- Assess fundal tone
- Perform bimanual massage if indicated
- Administer oxytocin, ergometrine, or misoprostol
- Begin IV fluids
- Transfer urgently
8.
4. Preterm Labour& PROM
Preterm Labour:
- Regular contractions before 37 weeks
- Cervical changes
PROM:
- Fluid leakage before onset of labor
- Confirm with speculum exam (avoid digital exams)
What to Do:
- Determine gestational age
- Assess for infection (fever, foul smell)
- Give steroids (dexamethasone) if <34 weeks
- Give antibiotics if PROM
- Refer for monitoring and possible delivery
9.
5. Puerperal Sepsis
Signs:
-Fever (>38°C)
- Foul-smelling lochia
- Lower abdominal pain
- Delayed involution of uterus
Risk Factors:
- Home deliveries
- Poor hygiene
- Retained products of conception
Management:
- Start broad-spectrum antibiotics (e.g., ampicillin + gentamicin + metronidazole)
- IV fluids
- Monitor vital signs
- Refer immediately if septic shock or poor response
10.
6. Decreased FetalMovements / Fetal Distress
History Taking Tips:
- “When did you last feel the baby move?”
- “How many times does it move in a day?”
Assessment:
- Listen for fetal heart tones (Doptone or Pinard horn)
- If unavailable, assess clinically (palpate movements)
Action:
- Refer urgently for USS and CTG
- Do not delay if fetal movements have stopped
11.
Essential Supplies inour Clinic
- Oxytocin, Ergometrine, Misoprostol
- Magnesium Sulfate (for eclampsia)
- Labetalol/Hydralazine (for BP control)
- Dexamethasone (for preterm labor)
- Ampicillin/Gentamicin/Metronidazole
- IV fluids and cannulas
- Gloves, clean delivery kits
- BP machine and stethoscope
- Doppler or Pinard horn
CC:
Bilateral lower limbswelling x 4/7
Headaches x 2/7
Epigastric pains x 1/7
HPI
M.M presented with 4-day hx of progressive painless bilateral L.L
swelling. 2 days later she developed persistent frontal headaches, on
and off, refractory to paracetamol. A day prior to presentation, she
experienced sharp epigastric pains radiating to the RUQ
accompanied by mild visual blurring and generalized body
weakness. Her BP recorded in 1st
trimester at 8wks gestation was
120/70mmHg. Has no known hx of chronic illness.
14.
• O/E: sicklooking, afebrile, not in obvious resp distress
• VITALS
BP- 172/120mmHg PR-102bpm SPo2- 97%
P/A
Gravid, with tender epigastrium, no palpable contractions
FH-28wks, FHR-144bpm, Lie- transverse, Presentation- Breech
Has pedal edema up to the level of the ankles
15.
LAB WORKS
FHG- NOSIGNIFICANT FINDING
URINALYSIS – Protein 2+
UECS- Normal findings
LFTS- Normal results
16.
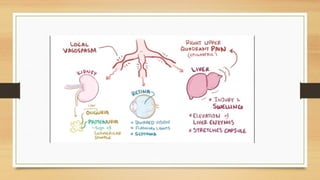
Pre-eclampsia
Pre-eclampsia is amultisystem disorder which occurs after 20 weeks of pregnancy
characterized by new-onset hypertension (BP- >140/90) with proteinuria ((≥0.3
g/day or dipstick ≥1+) and/or organ dysfunction
Spectrum of hypertensive disorders that complicate pregnancy:
1. chronic hypertension,
2. preeclampsia superimposed on chronic hypertension,
3. gestational hypertension,
4. preeclampsia, and
5. eclampsia.
Risk factors
o Extremesof age (maternal age >35 yrs or <18 yrs)
o Black race
o Family history of preeclampsia
o Nulliparity
o Primigravida
o Preeclampsia in a previous pregnancy
o Change of male partner
o Diabetes
o Obesity
o Chronic hypertension o Renal disease
o Multiple gestation
21.
Essential for diagnosisof Pre-Eclampsia:
Hypertension: Hypertension is blood pressure (BP) of 140/90 mmHg or more on two occasions six hours apart
OR
A diastolic blood pressure of 110 mmHg or more on a single occasion
Proteinuria: Is a protein concentration of 0.3 g/I or more in at least two random urine specimens collected six
hours apart
OR
Urine dipstick finding of ‘trace’, ‘1+’, or more proteins Normally protein is not supposed to be present in urine.
Oedema: Gradual or sudden swelling of the face, hands and legs.
Eclampsia: It is a new onset of convulsions -fits (in the absence of other medical conditions predisposing to
convulsions) in a woman with pre-eclampsia.
22.
Impending Eclampsia
Symptoms andSigns of impending eclampsia include:
• Severe headache
• Drowsiness
• Mental confusion
• Visual disturbance (e.g. blurred vision, flashes of flight)
• Epigastric pain
• Nausea / vomiting
• A sharp rise in blood pressure
• Decreased urinary output
• Increased proteinuria Hyper-reflexia
23.
Progression to Eclampsia
Definition:
-Preeclampsia + seizures with no other known cause
Seizure Stages:
1. Tonic phase – stiffening
2. Clonic phase – jerking
3.Postictal phase – confusion/unconsciousness
Triggers:
- Uncontrolled hypertension
- Missed ANC visits
- Lack of seizure prophylaxis
24.
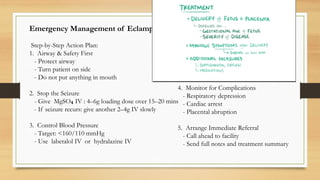
Emergency Management ofEclampsia (Outpatient)
Step-by-Step Action Plan:
1. Airway & Safety First
- Protect airway
- Turn patient on side
- Do not put anything in mouth
2. Stop the Seizure
- Give MgSO IV : 4–6g loading dose over 15–20 mins
₄
- If seizure recurs: give another 2–4g IV slowly
3. Control Blood Pressure
- Target: <160/110 mmHg
- Use labetalol IV or hydralazine IV
4. Monitor for Complications
- Respiratory depression
- Cardiac arrest
- Placental abruption
5. Arrange Immediate Referral
- Call ahead to facility
- Send full notes and treatment summary
25.
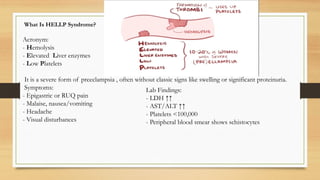
What Is HELLPSyndrome?
Acronym:
- Hemolysis
- Elevated Liver enzymes
- Low Platelets
It is a severe form of preeclampsia , often without classic signs like swelling or significant proteinuria.
Symptoms:
- Epigastric or RUQ pain
- Malaise, nausea/vomiting
- Headache
- Visual disturbances
Lab Findings:
- LDH ↑↑
- AST/ALT ↑↑
- Platelets <100,000
- Peripheral blood smear shows schistocytes
26.
Key Takeaways
Preeclampsiacan progress silently
Headache and visual changes are urgent
Epigastric pain ≠ GI issue — could be HELLP
Magnesium sulfate prevents and treats seizures
Don’t wait for labs — treat based on clinical suspicion
Timely referral saves lives
27.
References
- WHO Guidelineson Managing Obstetric Emergencies
- Kenya Ministry of Health Reproductive Health Manual
- MSD Manual, CDC Guidelines
- Jhpiego Maternal Health Resources