Downloaded 683 times

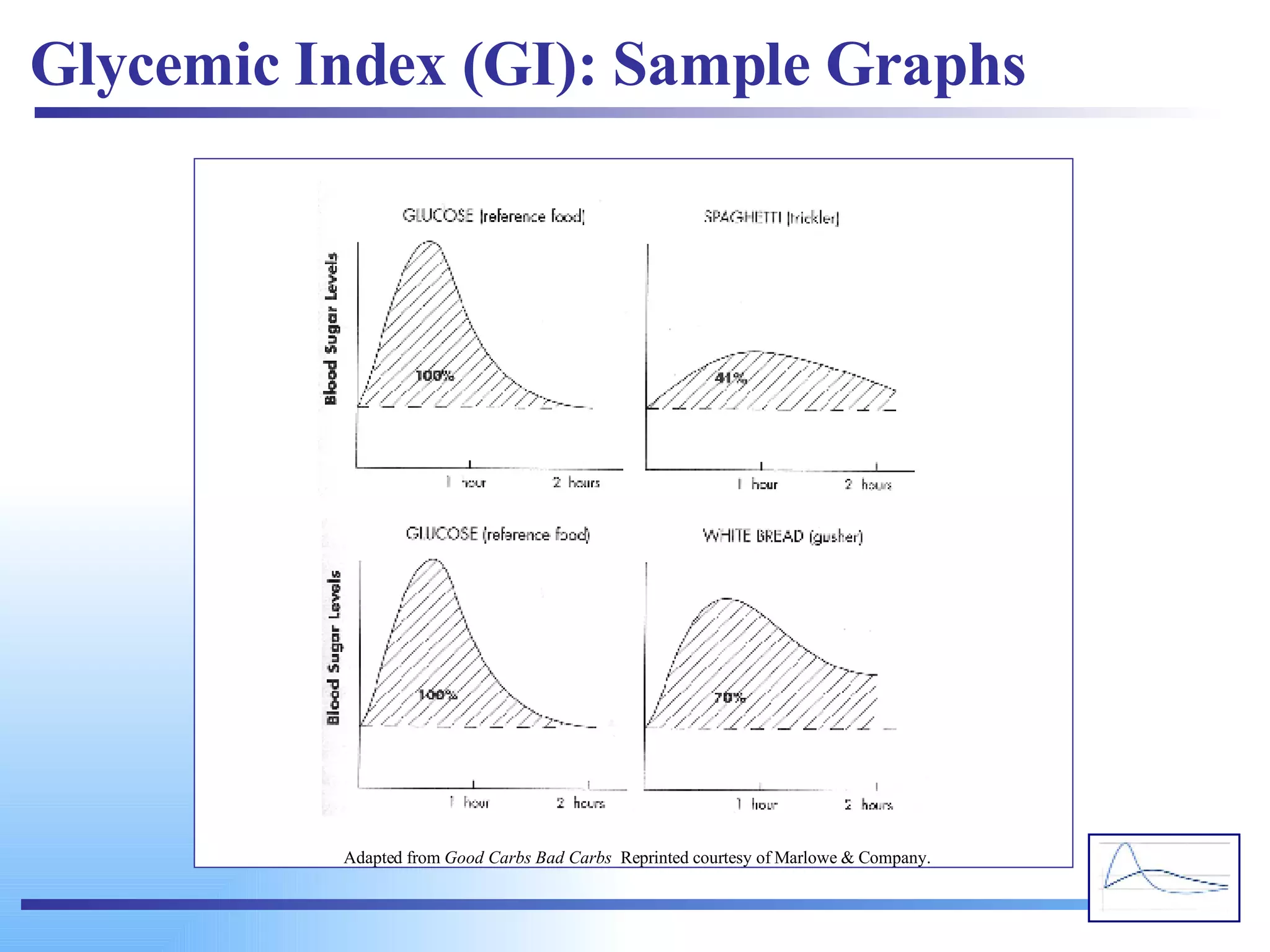





















![high glucose response (high GI) low glucose response (low GI) Plasma glucose response (mmol/L) from a high vs. low GI food. The change in blood glucose concentration over time is expressed and calculated as the area under the curve (AUC) (Wolever et al, 1991). www.glycemicindex.com [email_address]](https://image.slidesharecdn.com/glycemic-index2761/75/Glycemic-Index-60-2048.jpg)


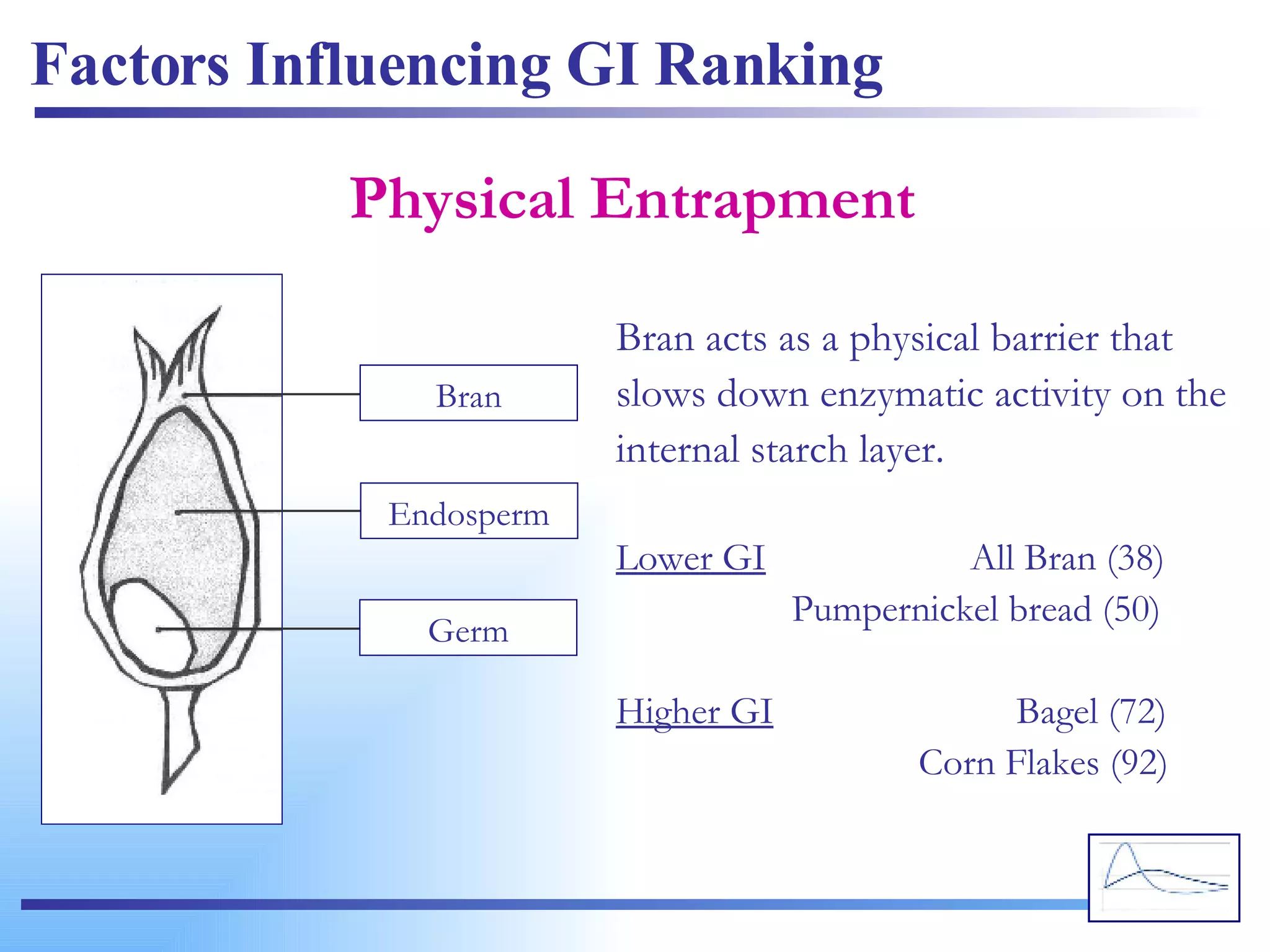
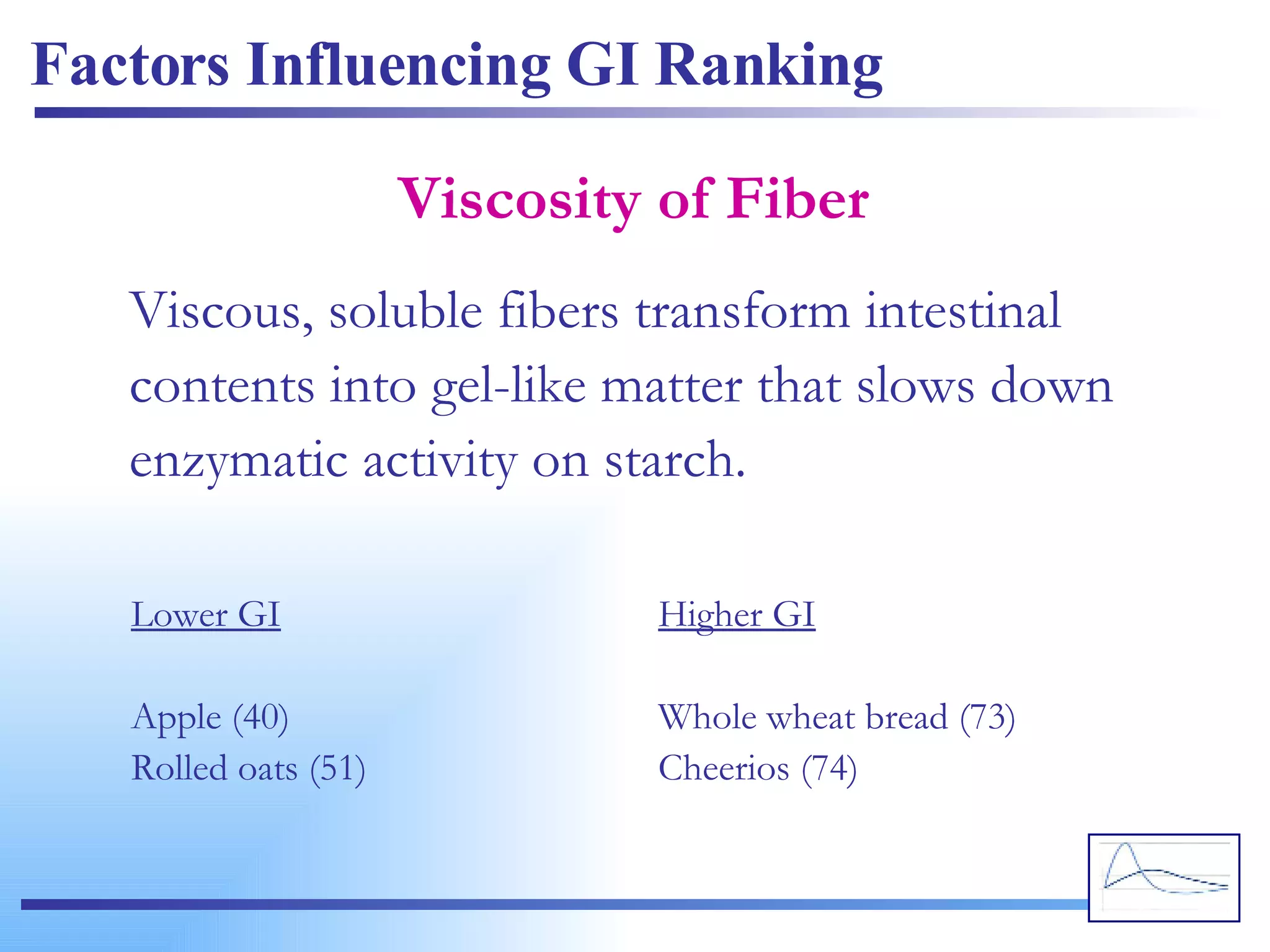
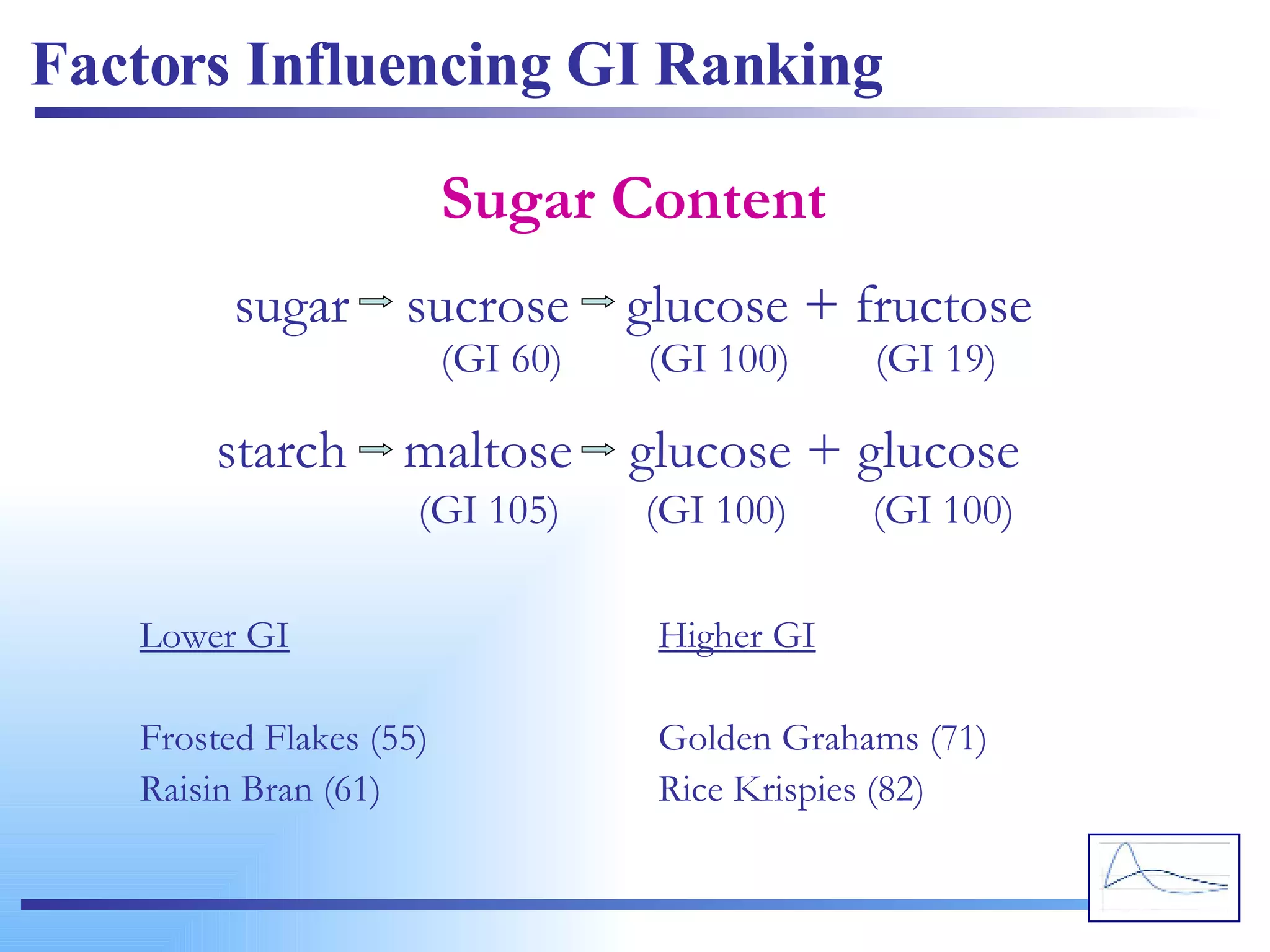
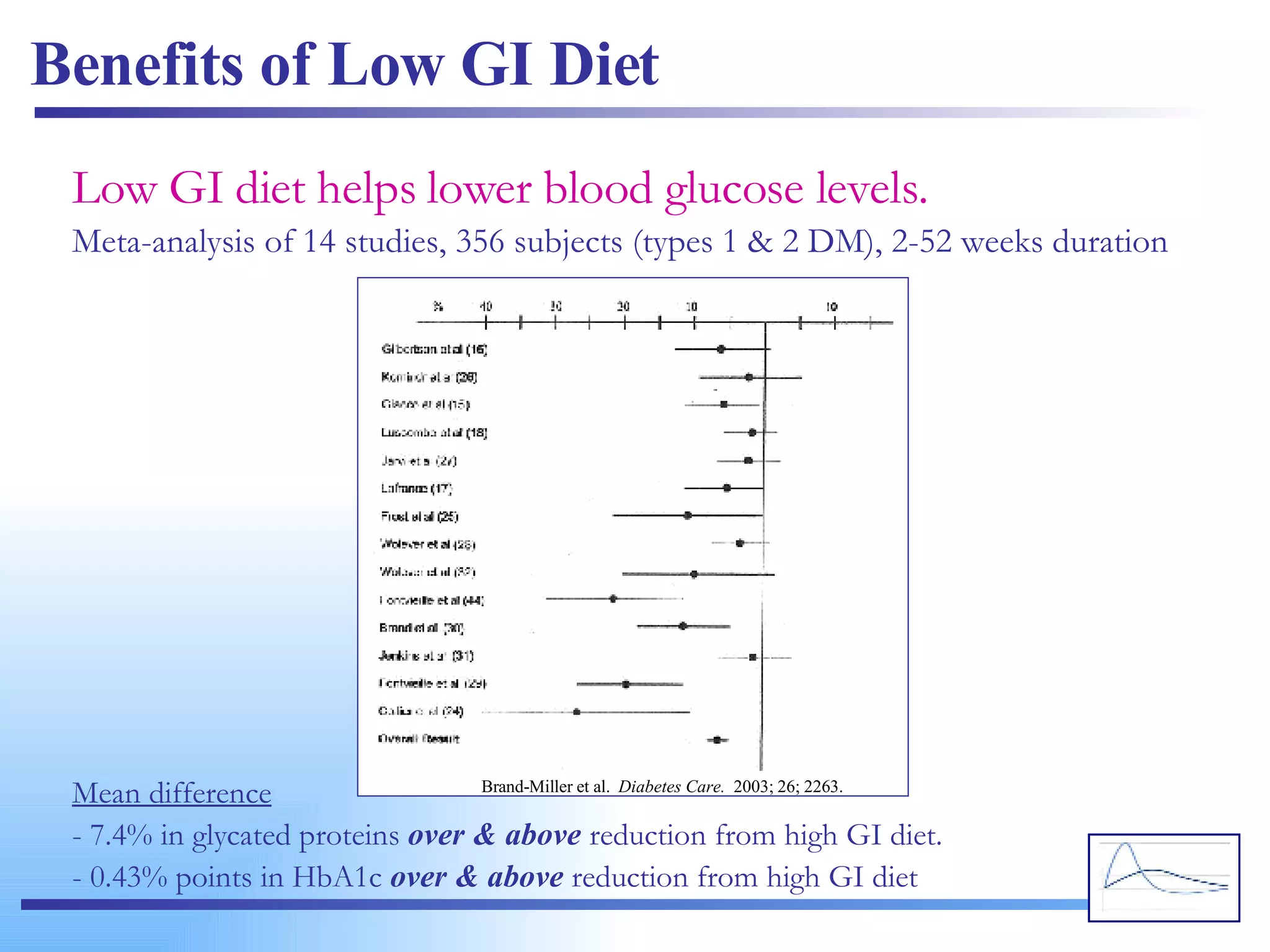
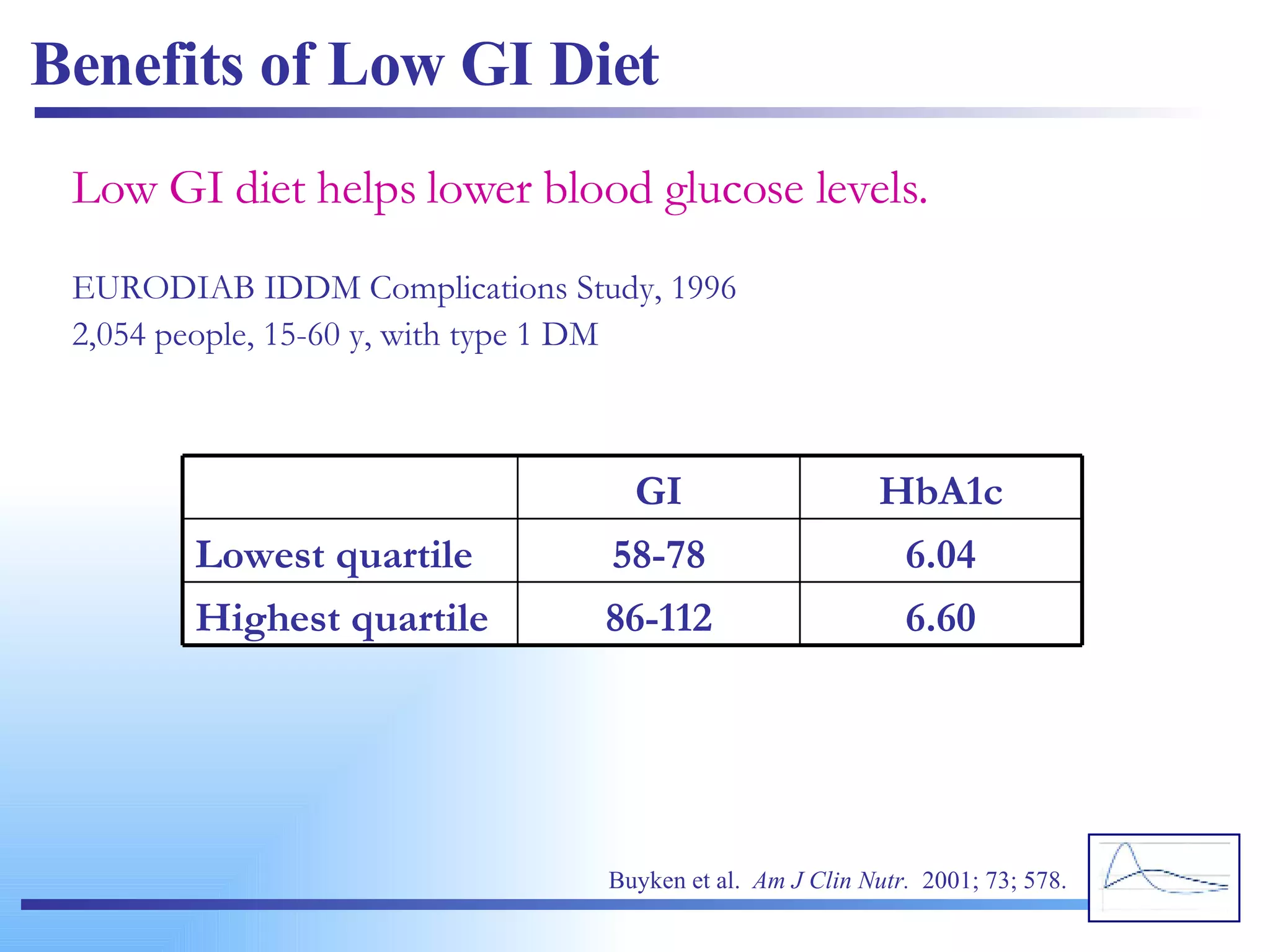
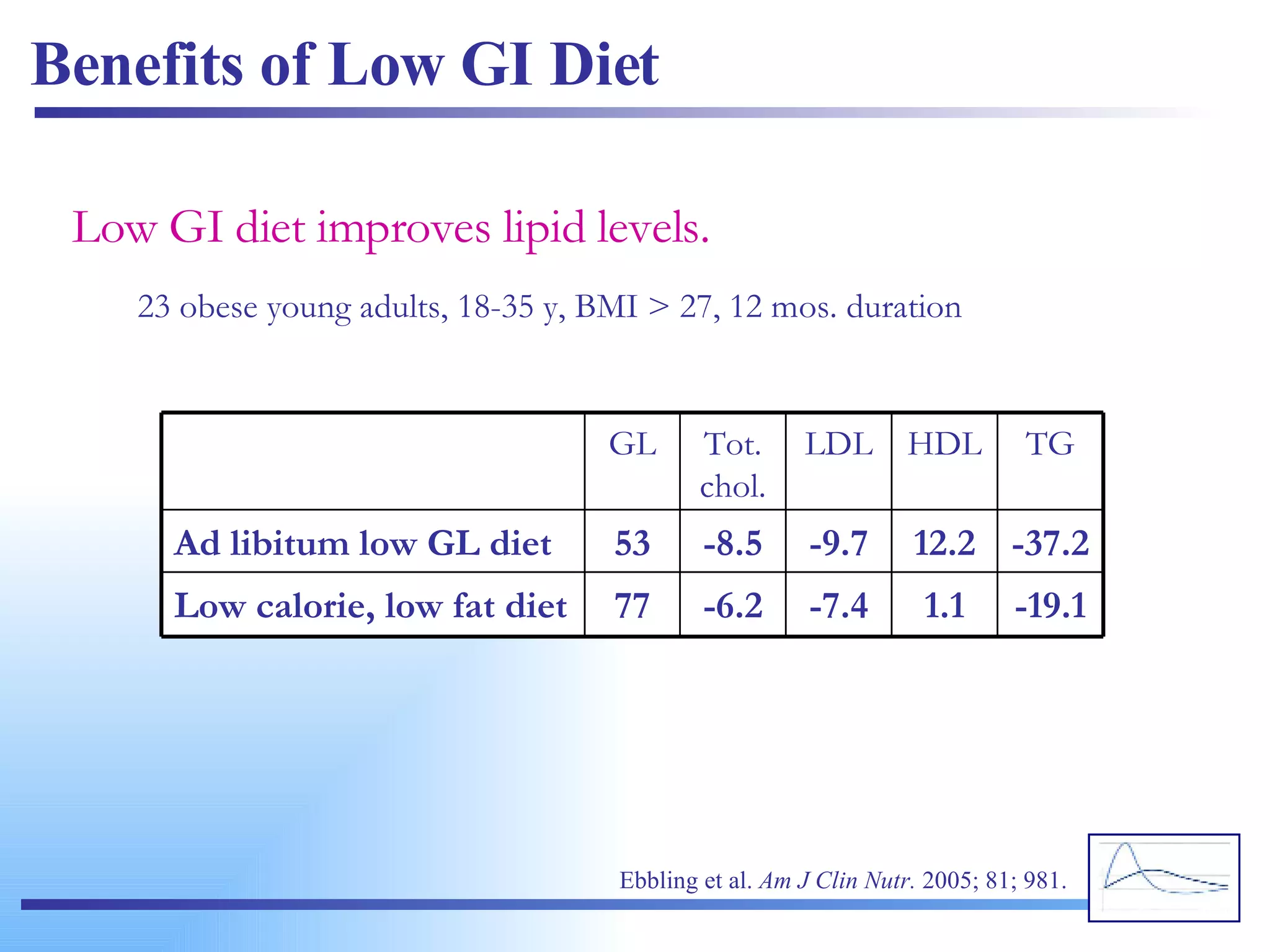
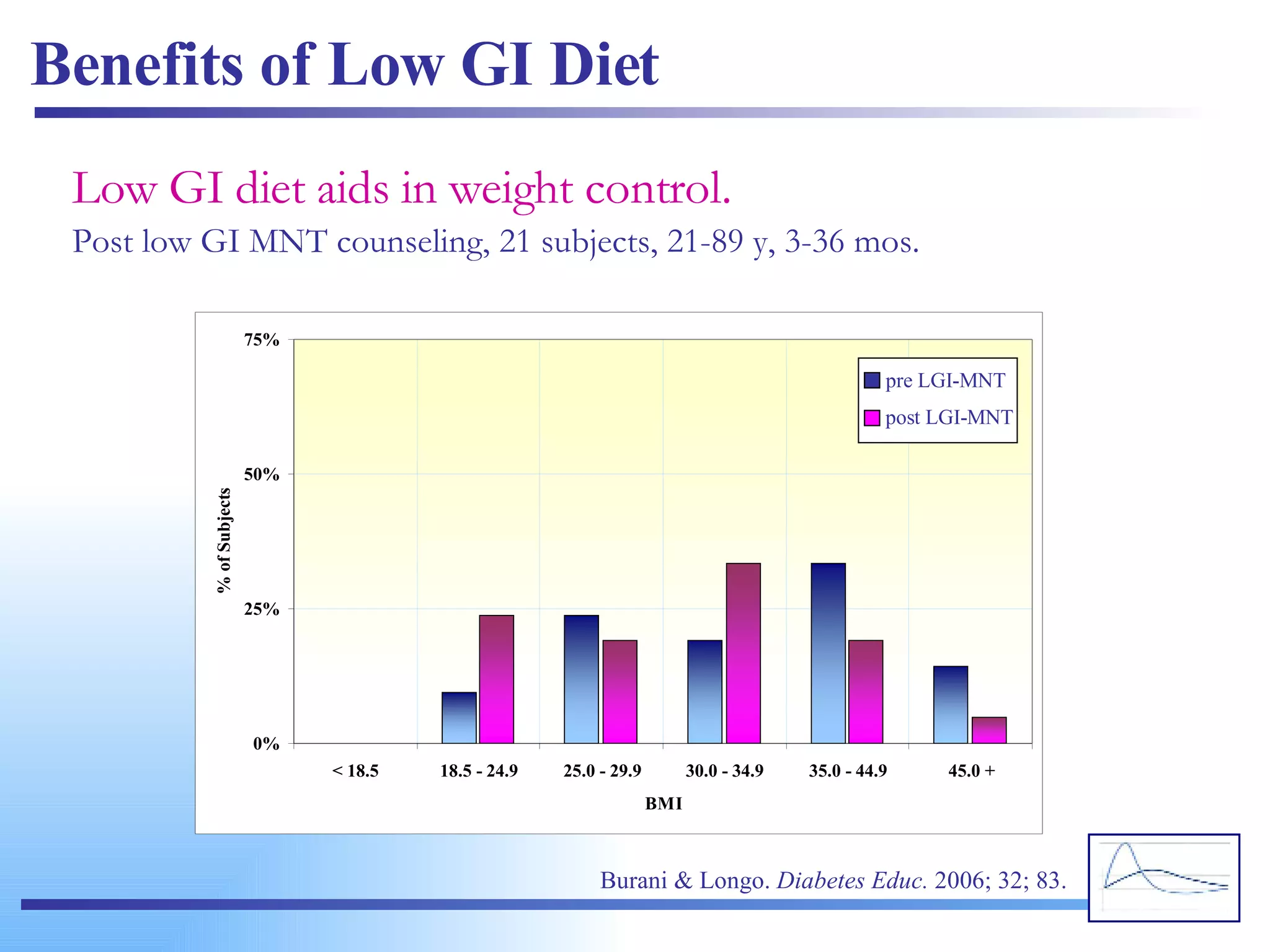
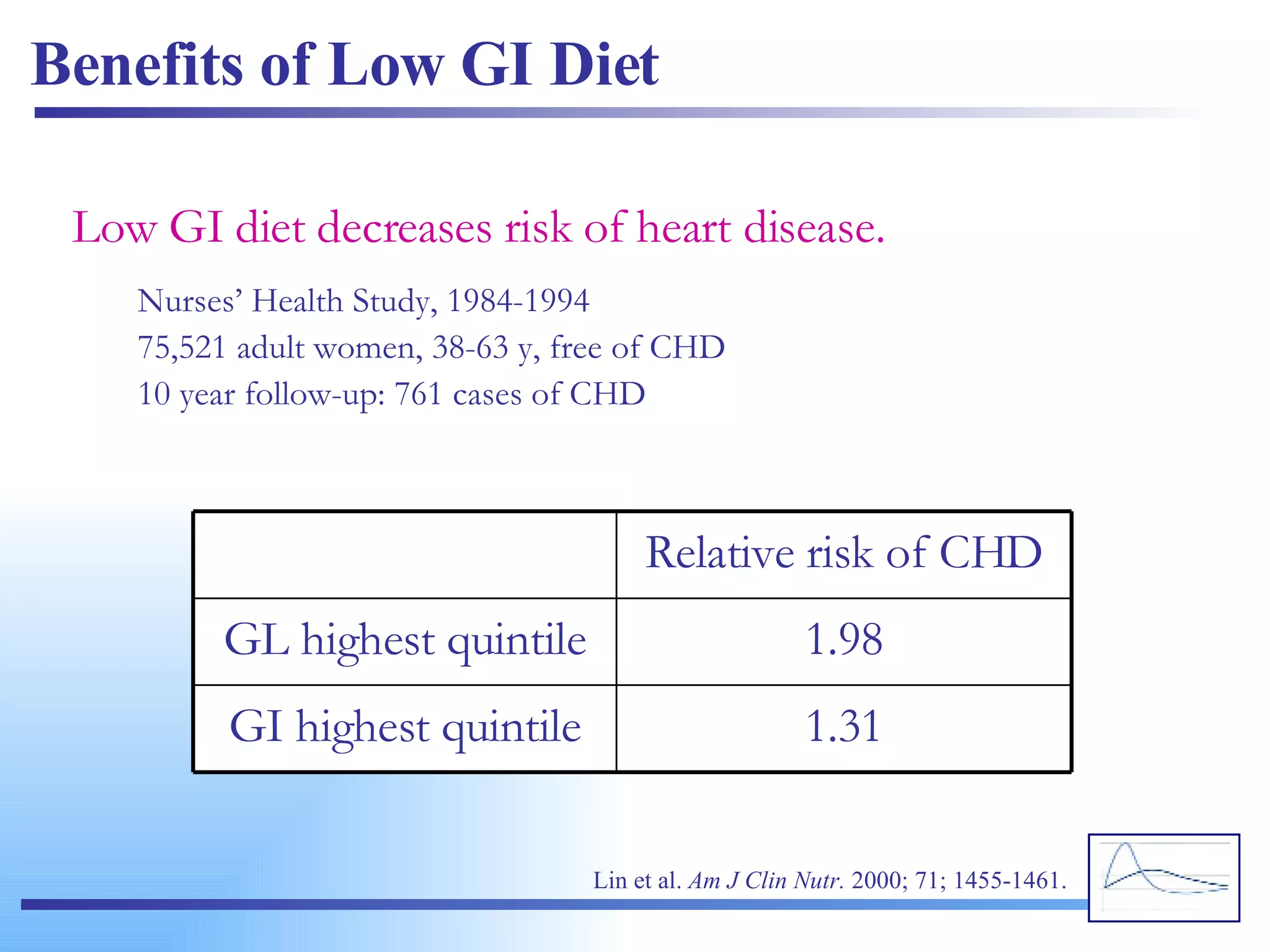
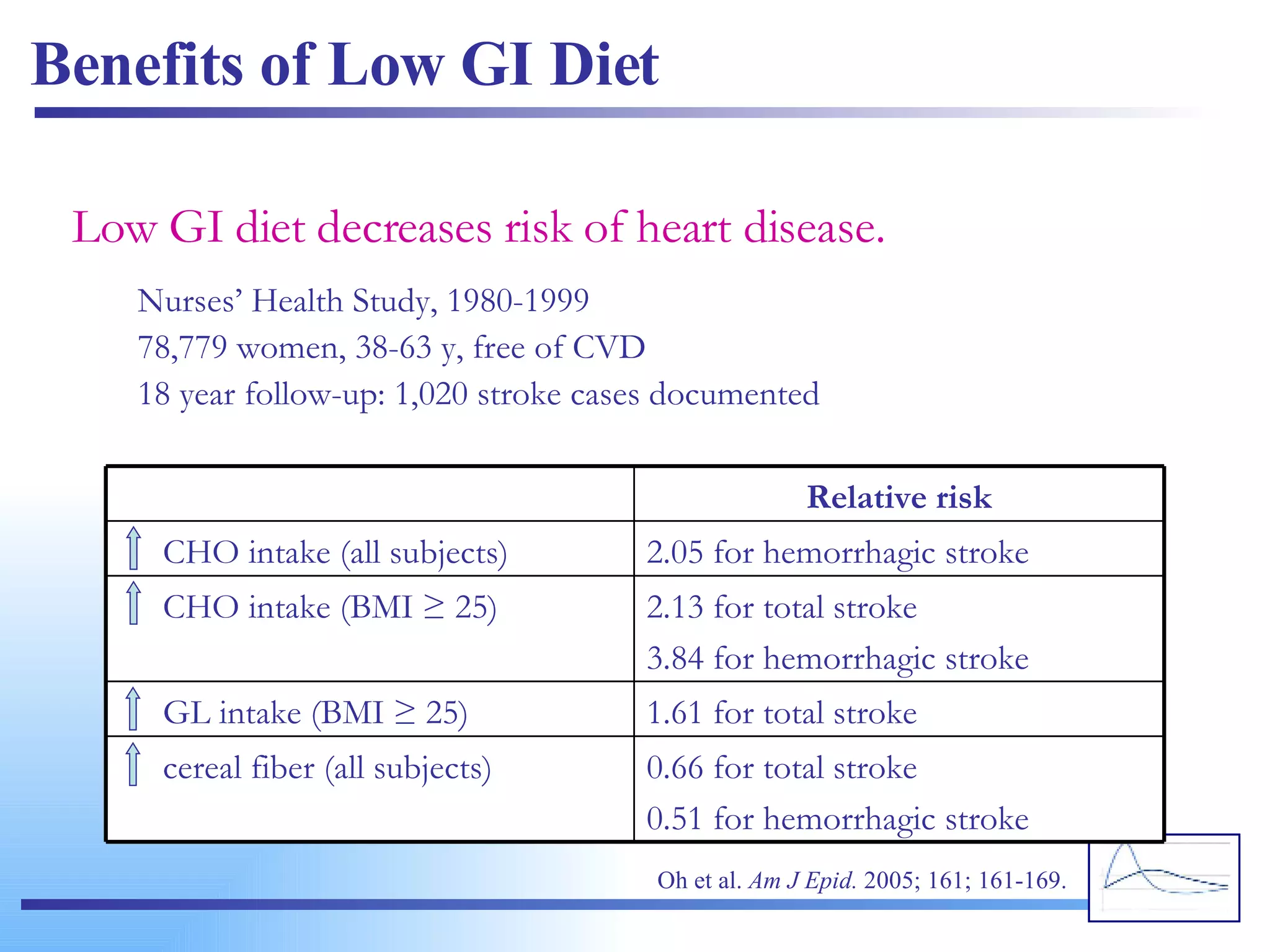
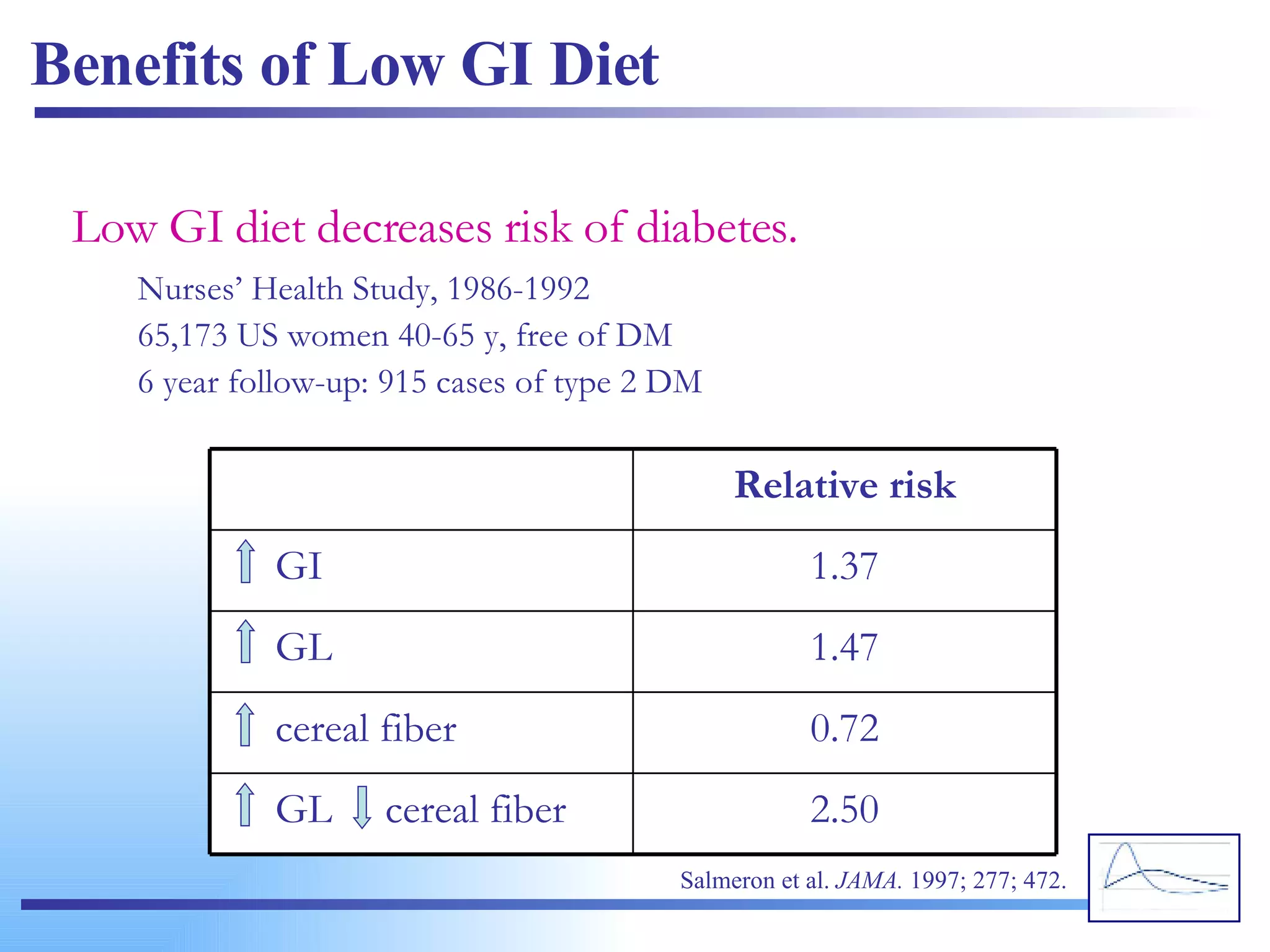
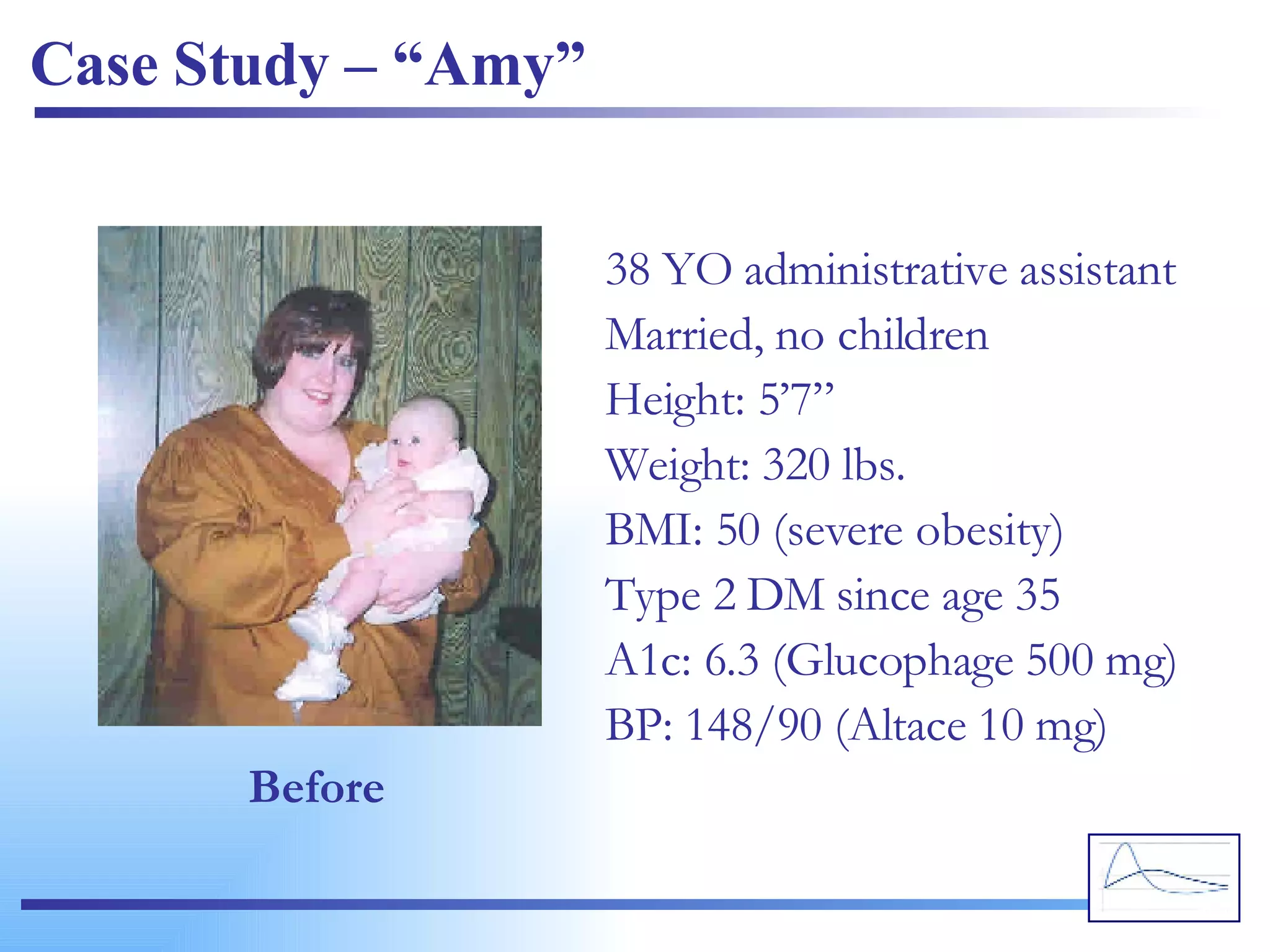
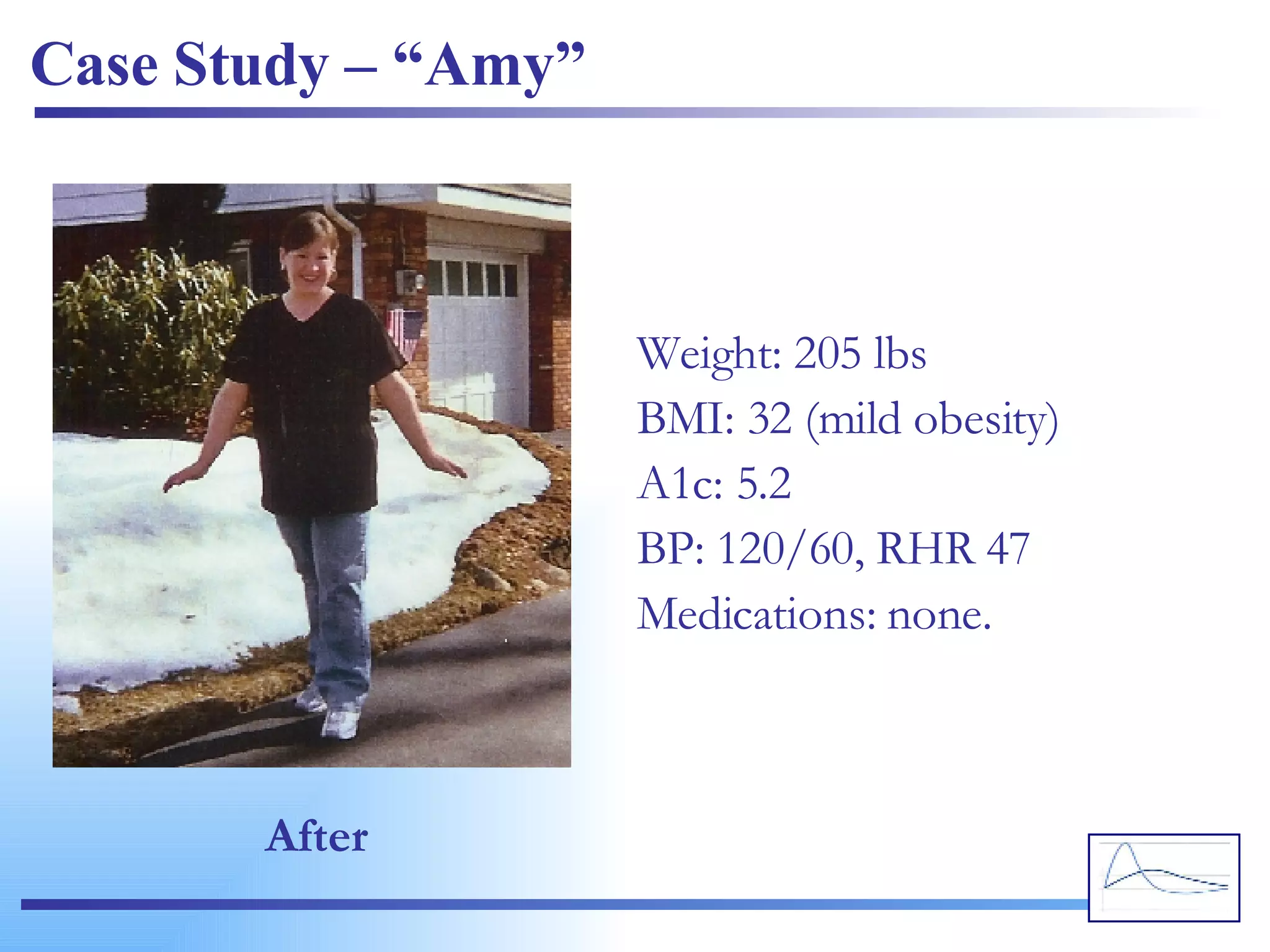
The document discusses the glycemic index (GI) and glycemic load (GL), explaining how different carbohydrates affect blood glucose levels and overall health. It outlines the factors influencing GI rankings of foods and presents the benefits of maintaining a low GI diet, such as improved blood glucose levels, weight control, and reduced risk of health issues like diabetes and heart disease. Additionally, it emphasizes the importance of a balanced diet while incorporating low GI foods and provides a case study demonstrating dietary changes and their positive effects.
















































![Best Ratbaggery for 2019 so far... [A personal selection of comics]](https://cdn.slidesharecdn.com/ss_thumbnails/ratbagslides2019pdf-190705124520-thumbnail.jpg?width=640&height=640&fit=bounds)





































