Downloaded 47 times






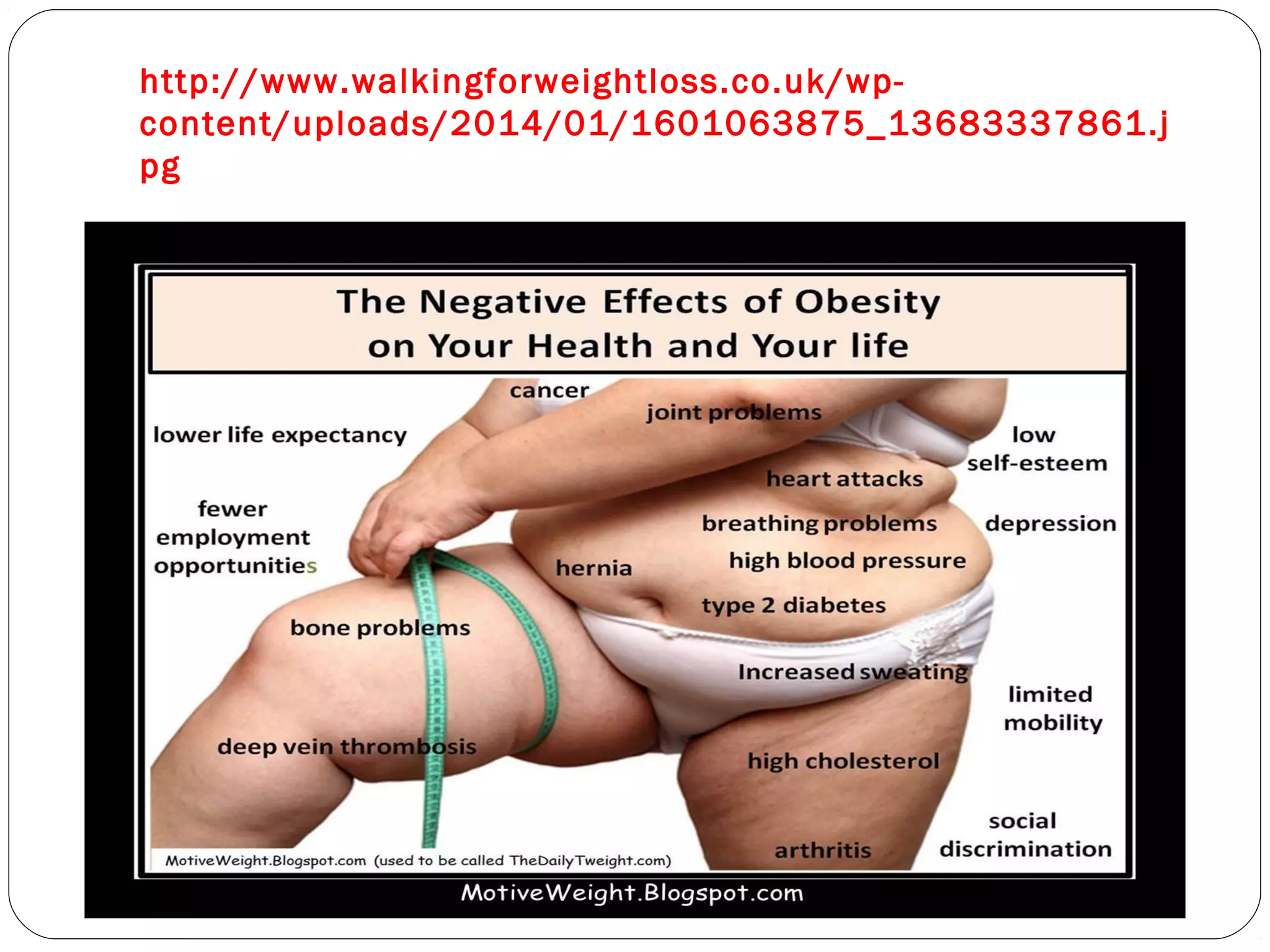
































The document outlines the rising prevalence and health risks associated with obesity, defining it primarily through BMI and highlighting the need for comprehensive management strategies. Current treatments include behavioral changes, medications, and surgical options, although drugs often have limited efficacy and side effects. The author emphasizes the necessity for a deeper understanding of the underlying mechanisms of obesity to achieve effective and lasting solutions.






























































































