Downloaded 17 times


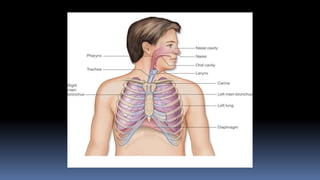


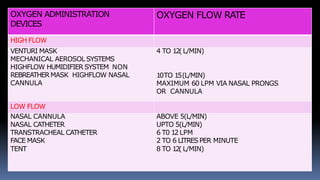
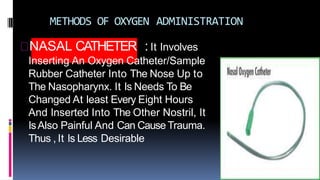

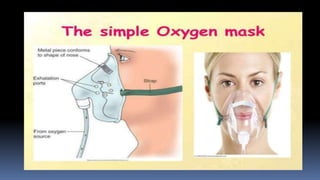

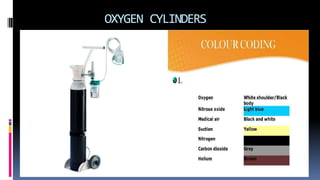
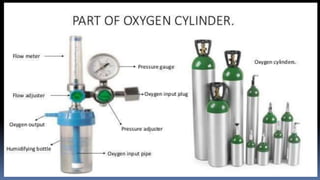



Oxygenation is the process of oxygen delivery to tissues through respiration. Oxygen therapy provides supplemental oxygen to patients through various devices to treat hypoxemia and hypoxia. It aims to facilitate normal tissue metabolism and correct low blood oxygen levels. Factors like physiological changes, development, lifestyle, and environment can impact oxygenation. The document outlines oxygen administration devices, methods of delivery including nasal cannulas and masks, and the steps for proper oxygen therapy preparation, procedure, and aftercare of patients and equipment.






















































































