This document provides an overview of different types of nystagmus, including:
- Physiological nystagmus like optokinetic nystagmus
- Pathological nystagmus like infantile nystagmus syndrome
- Characteristics used to classify nystagmus like plane, amplitude and frequency
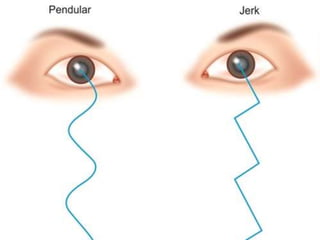
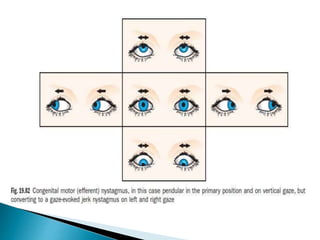
- Specific types like jerk nystagmus, pendular nystagmus, and factors that can induce or alleviate nystagmus.
Treatment options for some types are also mentioned, such as contact lenses and eye muscle surgery.