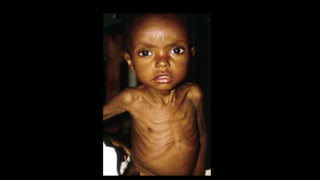
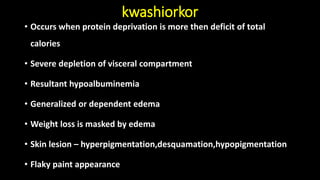
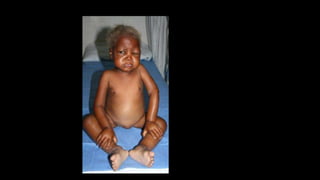
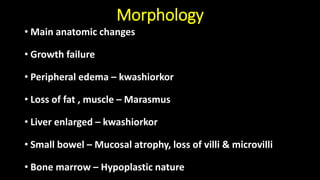
Nutritional disease refers to protein energy malnutrition (PEM), which results from inadequate intake of proteins and calories. PEM causes deficiencies in digestion and absorption, resulting in loss of fat, muscle tissue, weight loss and general weakness. PEM is a serious and often lethal condition, especially in children under 5 years old. It has various etiologies including poverty, infections, illness, alcoholism and dietary restrictions. PEM is diagnosed using measurements like body mass index, mid-arm circumference and serum protein levels. The two main types are marasmus, characterized by weight loss and muscle depletion, and kwashiorkor, distinguished by edema and hypoalbuminemia.