Downloaded 14 times


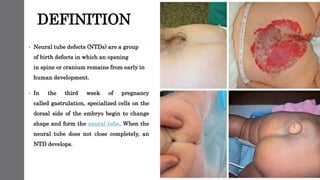
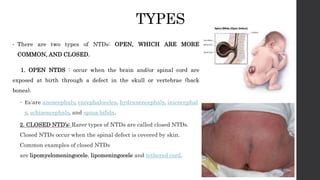

This document discusses neural tube defects (NTDs), which are birth defects where an opening remains in the spine or skull early in development. The main types are open defects like spina bifida and anencephaly, and closed defects. NTDs can be caused by folic acid deficiency, genetics, medications, and other factors. Symptoms vary depending on the specific defect. Diagnosis may involve ultrasounds and alpha-fetoprotein testing. Treatment ranges from surgery to palliative care, while prevention focuses on adequate folic acid intake before and during pregnancy.



































![Neural tube defect [ntd]](https://cdn.slidesharecdn.com/ss_thumbnails/neuraltubedefectntd-170814055941-thumbnail.jpg?width=640&height=640&fit=bounds)






















![Human genome project [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/humangenomeprojectautosaved-210929062307-thumbnail.jpg?width=640&height=640&fit=bounds)




























