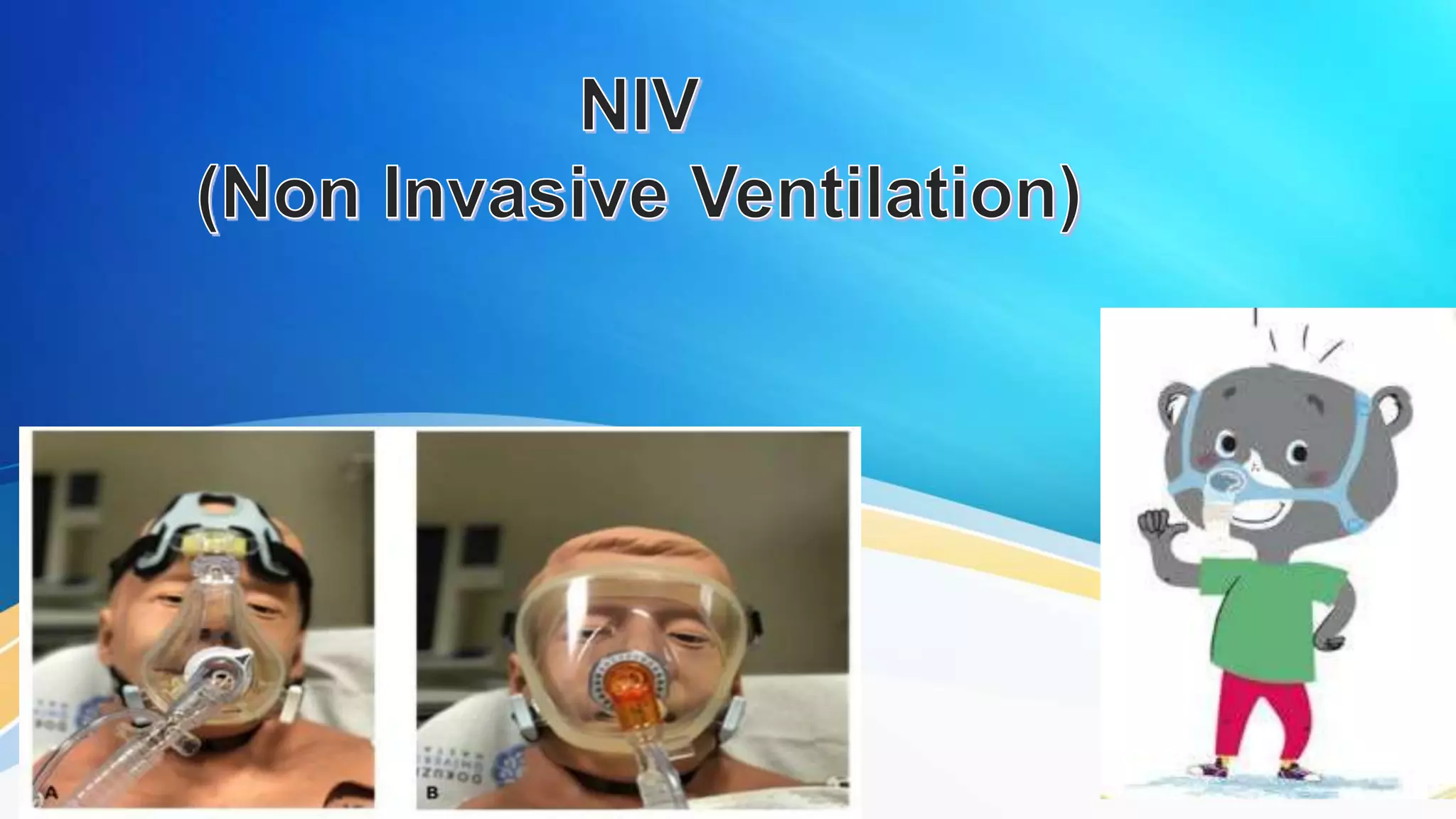
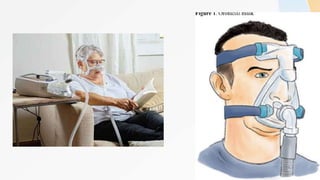
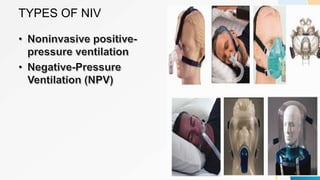
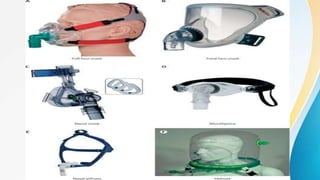
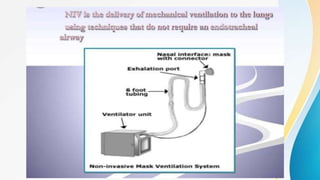
This document discusses non-invasive ventilation (NIV) and its use in treating respiratory conditions. NIV delivers oxygen through a face mask, avoiding the need for an endotracheal tube. It works by creating positive airway pressure, reducing breathing effort and expanding the lungs. The main types of NIV are noninvasive positive pressure ventilation using interfaces like masks, and negative pressure ventilation employing devices like iron lungs. Contraindications and instructions for use are also outlined.






























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








