Downloaded 23 times

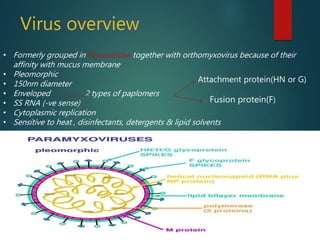





Newcastle disease is a contagious viral disease of birds caused by avian paramyxovirus-1. It is transmitted through contact with infected birds or their feces/secretions. Clinical signs include respiratory, neurological and intestinal symptoms with high mortality in some strains. Diagnosis involves virus isolation from samples and serological tests. Control relies on vaccination, biosecurity, and culling infected flocks.



















































































