Downloaded 332 times





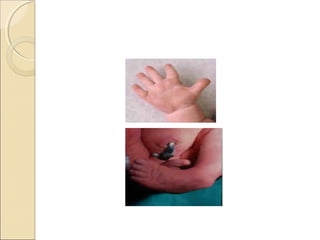


The document discusses essential newborn care including keeping the newborn warm through skin-to-skin contact, early and exclusive breastfeeding within the first hour of birth, eye care through prophylaxis to prevent ophthalmia neonatorum, and clinical assessment of the newborn to check for any problems after delivery. Key interventions like clean delivery, resuscitation if needed, immunization, and management of preterm or low birth weight babies are also described. The goal of essential newborn care is to ensure the health of the newborn during the critical first days and week of life.














































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








