Downloaded 110 times

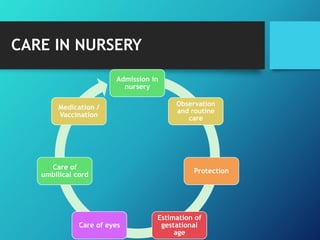

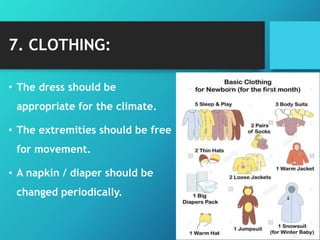

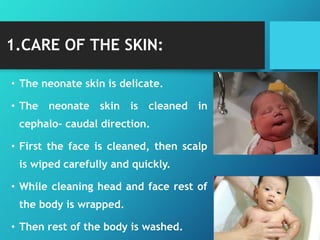

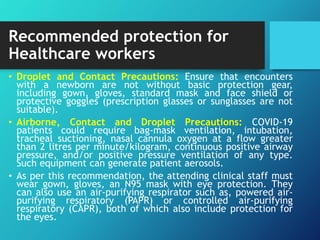

The document outlines essential newborn care practices emphasizing the role of maternal involvement and early bonding between mother and baby. It addresses the crucial first 24 hours of a newborn's life, detailing immediate care procedures, monitoring for congenital issues, and ensuring proper nutrition and infection control. It also incorporates guidelines for managing newborns during the COVID-19 pandemic, highlighting infection prevention, neonatal resuscitation, and vaccination protocols.































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)



