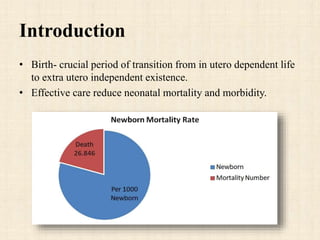
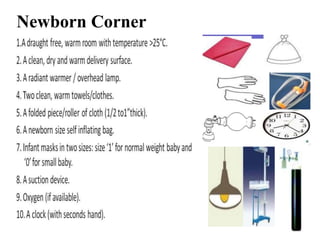
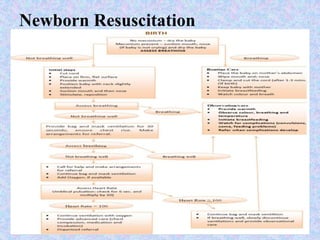
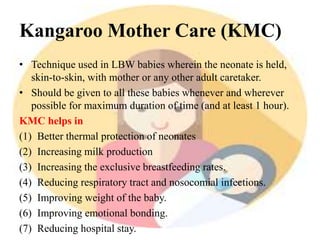
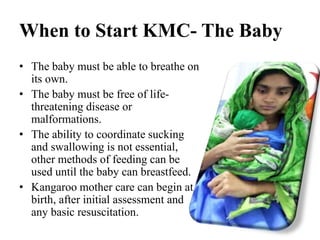
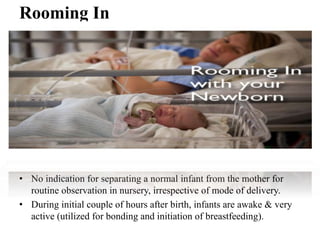
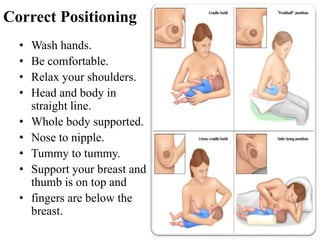
The document outlines essential newborn care, emphasizing the importance of effective care during the neonatal period to reduce mortality and morbidity. It details components such as temperature control, feeding practices, hygiene, and identification of danger signs, while providing guidelines for immediate post-birth care including resuscitation and cord management. Additional aspects include breastfeeding initiation, developmental monitoring, and the significance of mother-infant bonding through techniques like kangaroo care.