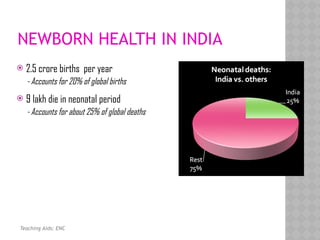
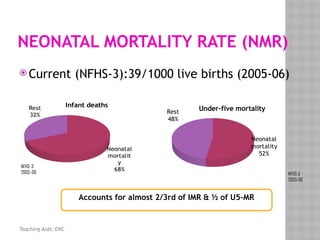
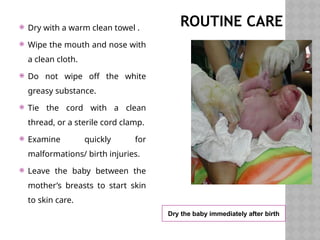
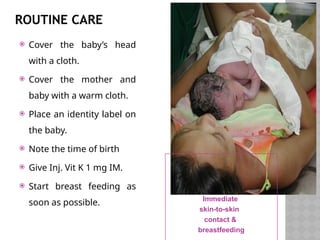
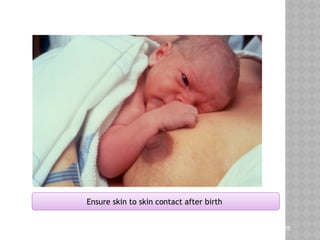
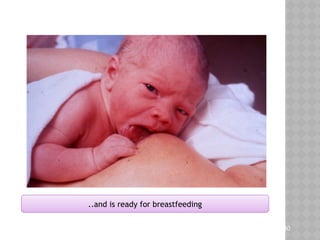
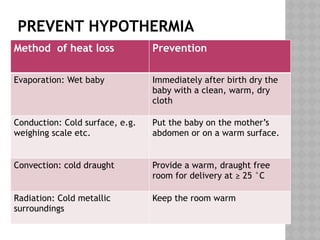
The document covers essential newborn care practices, including management at birth, neonatal resuscitation, and addressing common neonatal problems. It highlights the high neonatal mortality rate in India, with leading causes being infections, asphyxia, and prematurity, and emphasizes the importance of skilled care during delivery and early breastfeeding. Key practices include maintaining cleanliness, preventing hypothermia, and ensuring timely medical evaluations for congenital anomalies.