Definition
Neonatal jaundiceis a term used when a
newborn has yellow coloration of the skin
and sclera as the result of accumulation of
bilirubin.
Jaundice is the most common condition
that requires medical attention in newborns.
Mechanism of NeonatalJaundice
1.Over production of bilirubin:
8.8mg/kg/d in infants VS 3.8mg in adult
Increased RBC volume
Shorter RBC lifespan than adults(80 days
compared with 120 days)
Shunt bilirubin-from bone marrow ,liver
12.
Mechanism of NeonatalJaundice
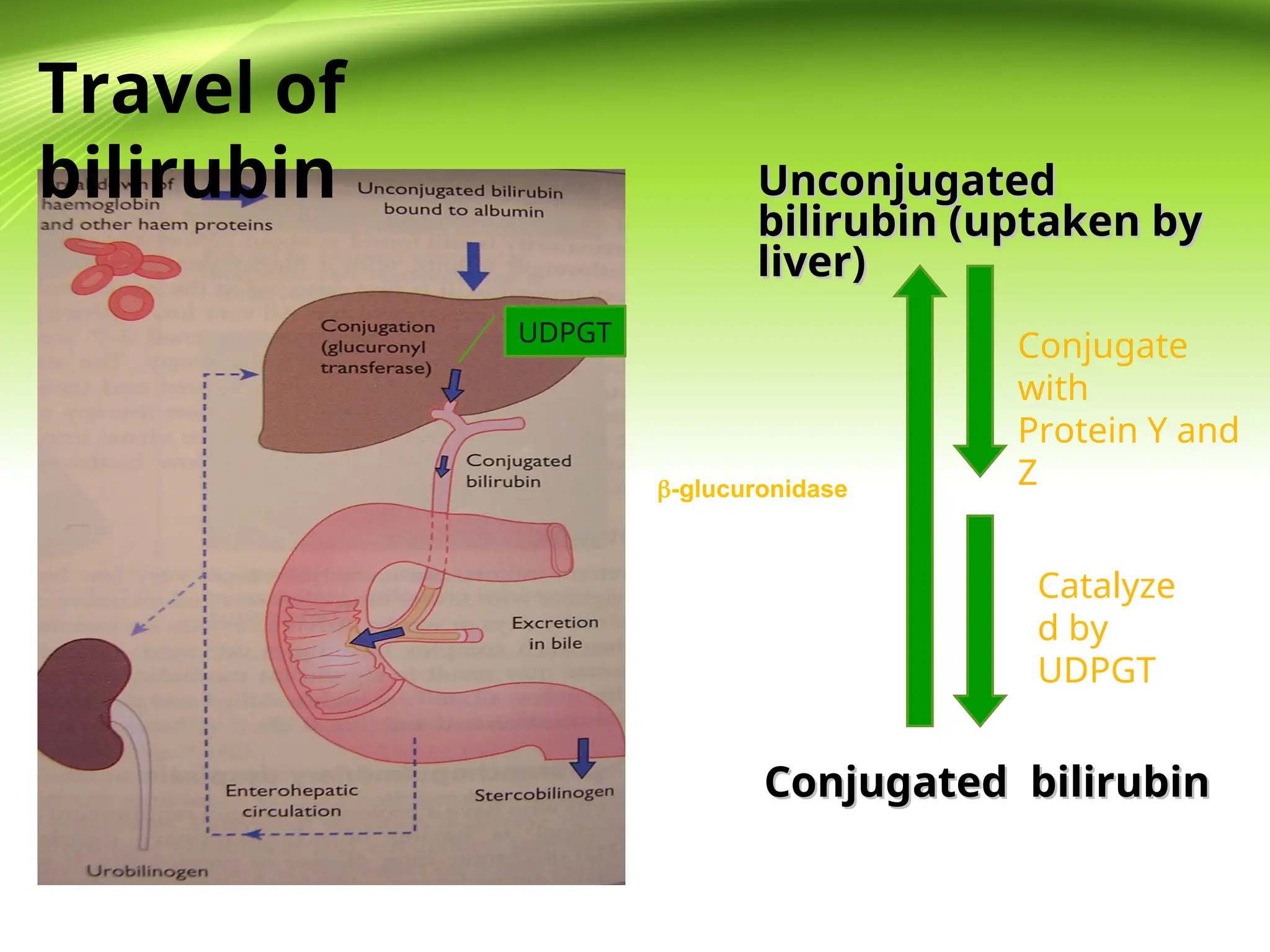
2.Transport of bilirubin is not enough
PH is intensively relative to the binding of
albumin to bilirubin (PH>7.4),but in newborns,PH
is always lower.
The albumin is the means of conveyance of
bilirubin from blood to the liver. Relative lower
concentration of serum albumin cause lower
transportation of bilirubin.
13.
Mechanism of NeonatalJaundice
3.Immaturity in metabolism in liver
Acceptor proteins Y,Z in lower level
Lower activity of uridine diphosphoglucurony1
transferase
14.
4. Increased enterohepaticcirculation
a. Poor peristalsis of intestine
b. Intestinal flora not established
c. Increased -glucuronidase activity
(Breast milk ) jaundice)
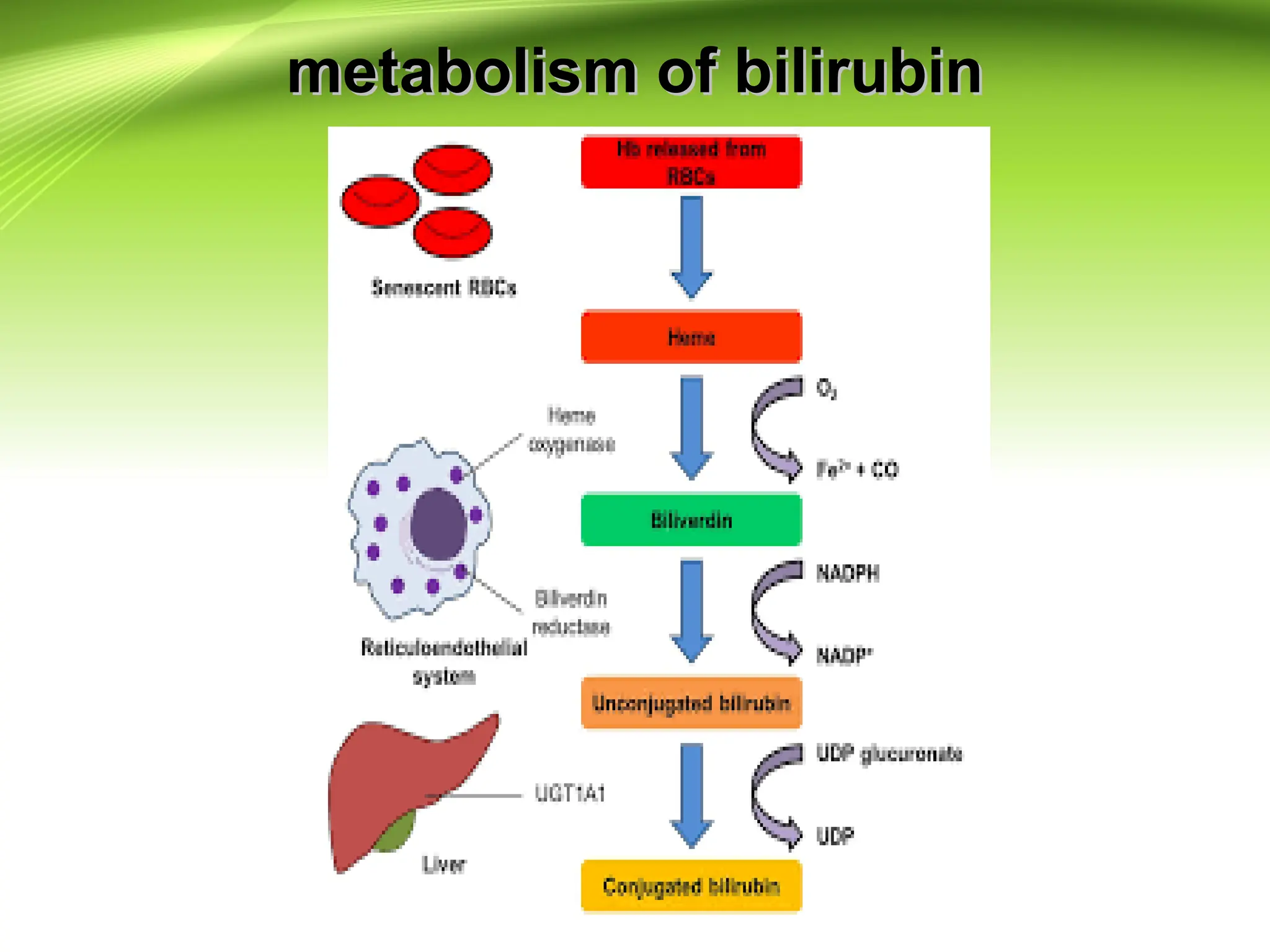
Conjugated bilirubin
Conjugated bilirubin
Unconjugated
Unconjugated
bilirubin
bilirubin
-glucuronidase
d. Delay of meconium
excretion
Mechanism of Neonatal Jaundice
15.
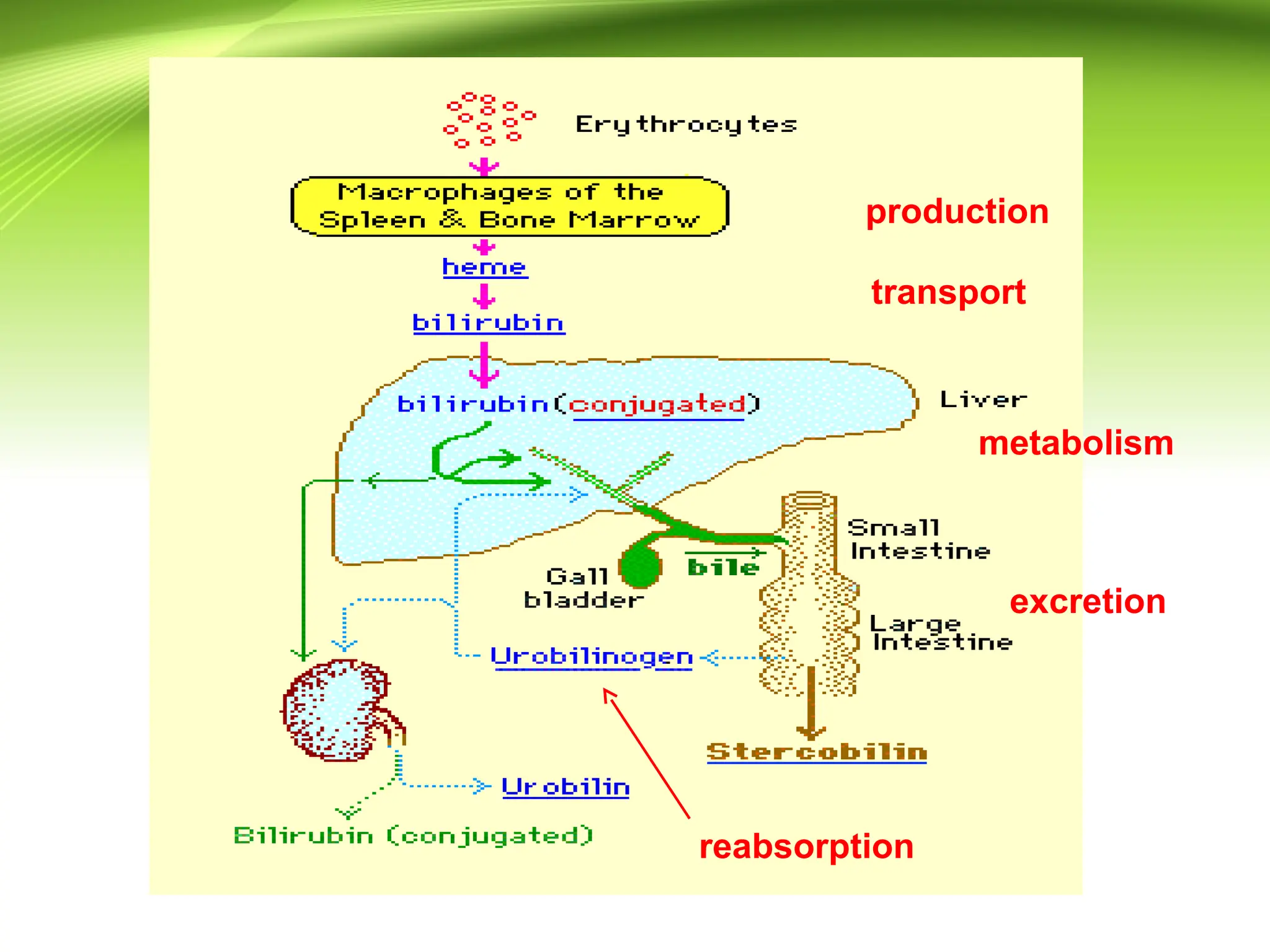
Pathophysiology
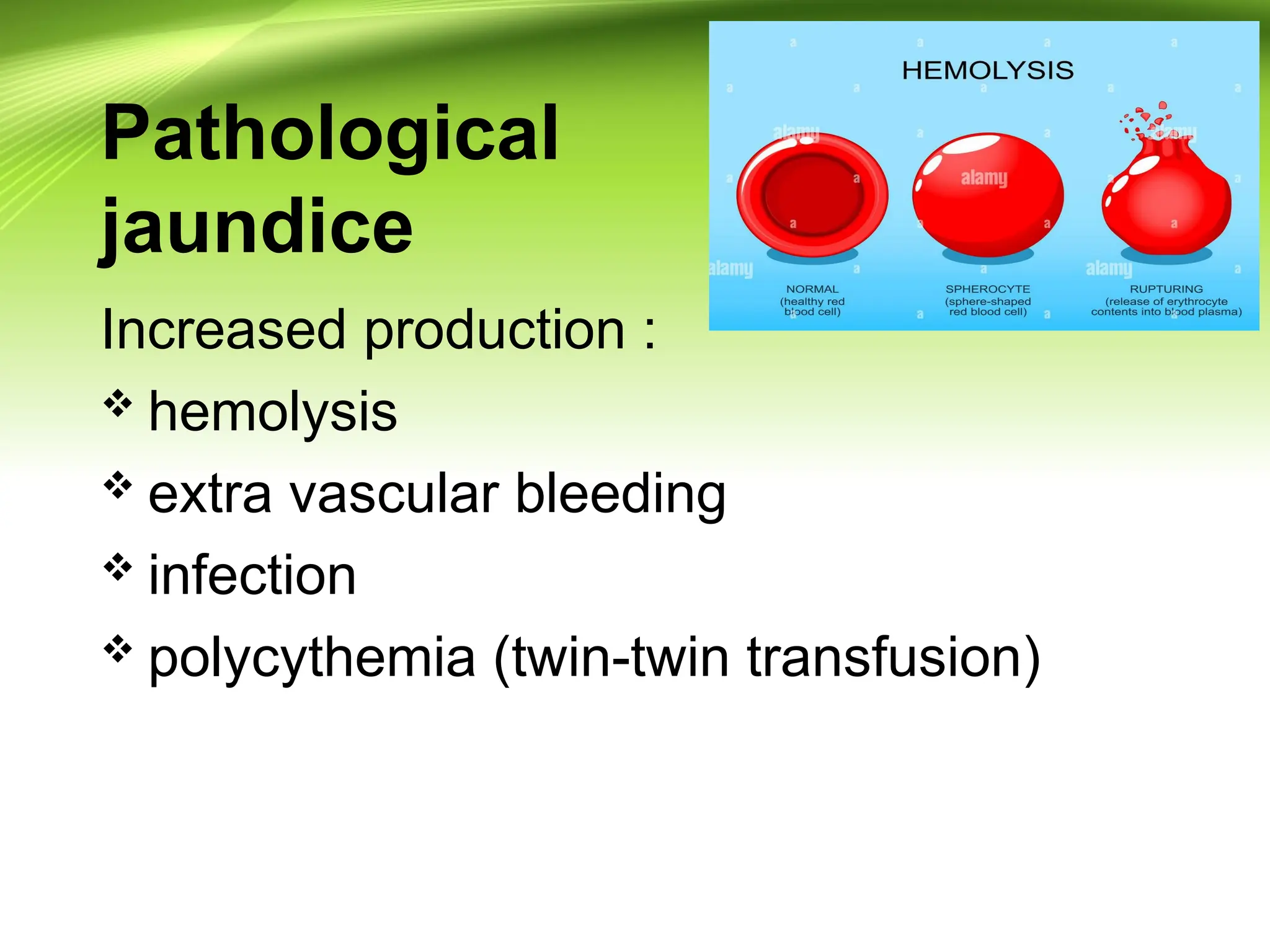
Increased bilirubinproduction
Decreased clearance of bilirubin
Decreased
Decreased
clearance
clearance
Increased
Increased
production
production
16.
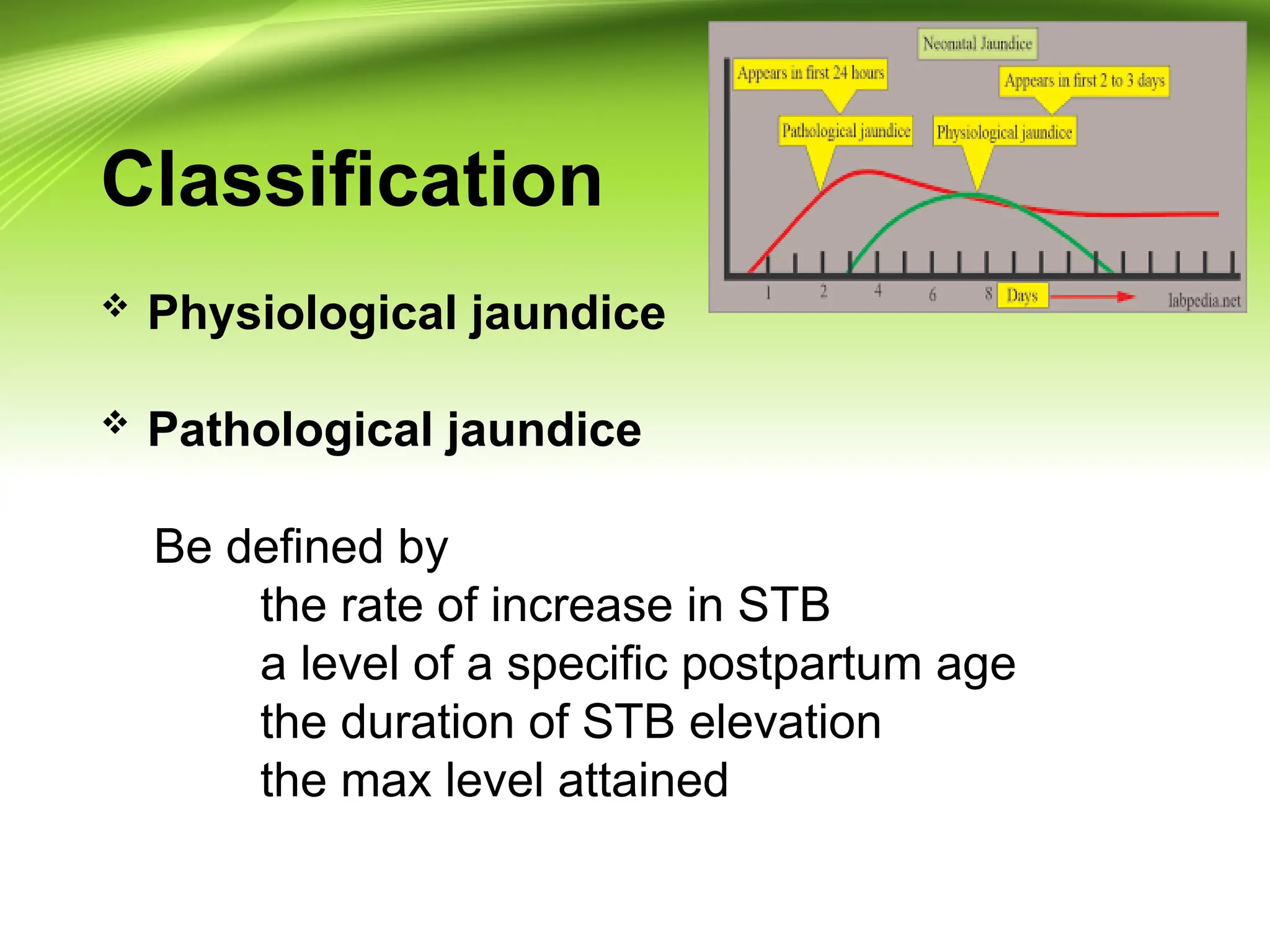
Classification
Physiological jaundice
Pathological jaundice
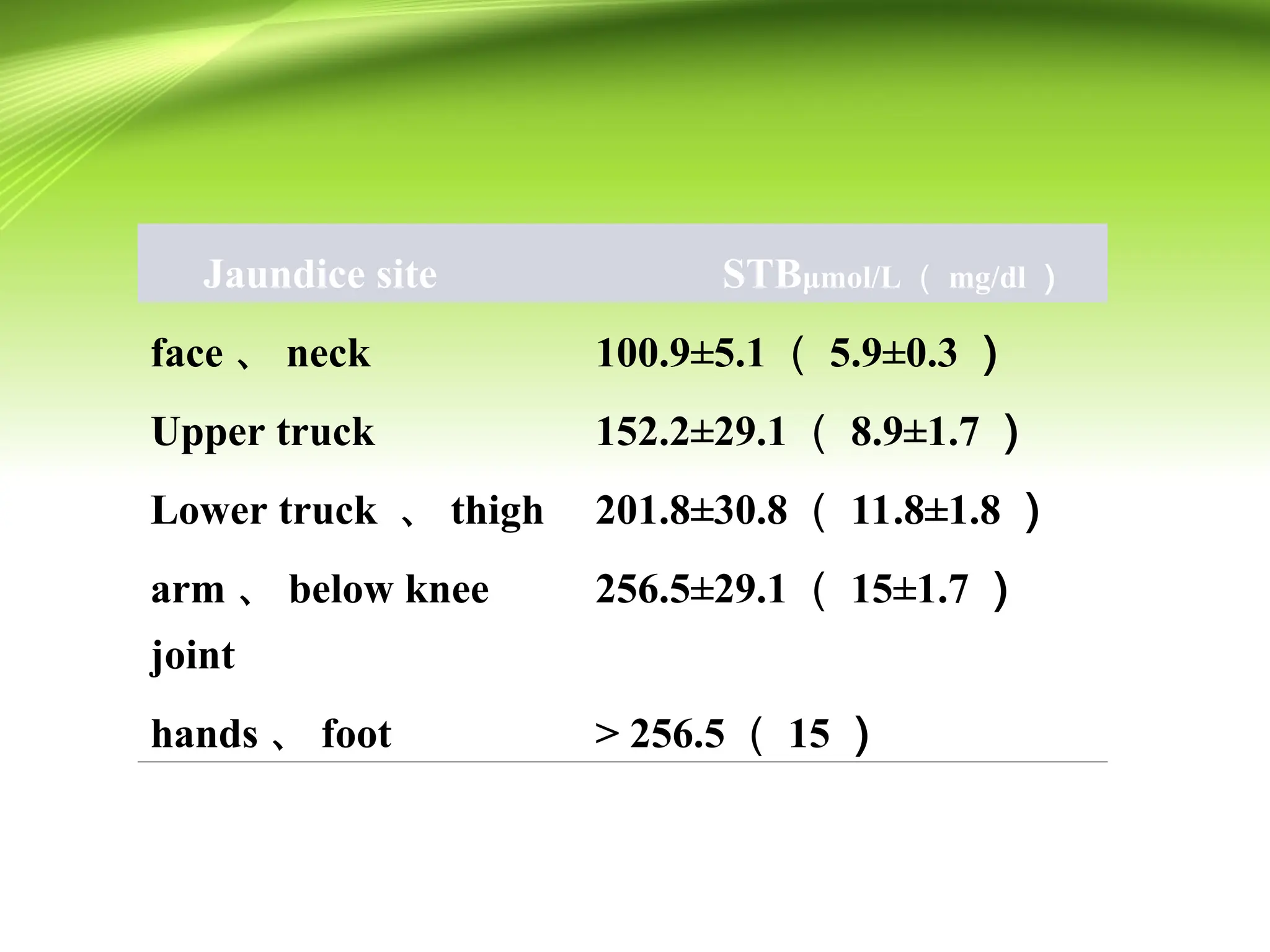
Be defined by
the rate of increase in STB
a level of a specific postpartum age
the duration of STB elevation
the max level attained
17.
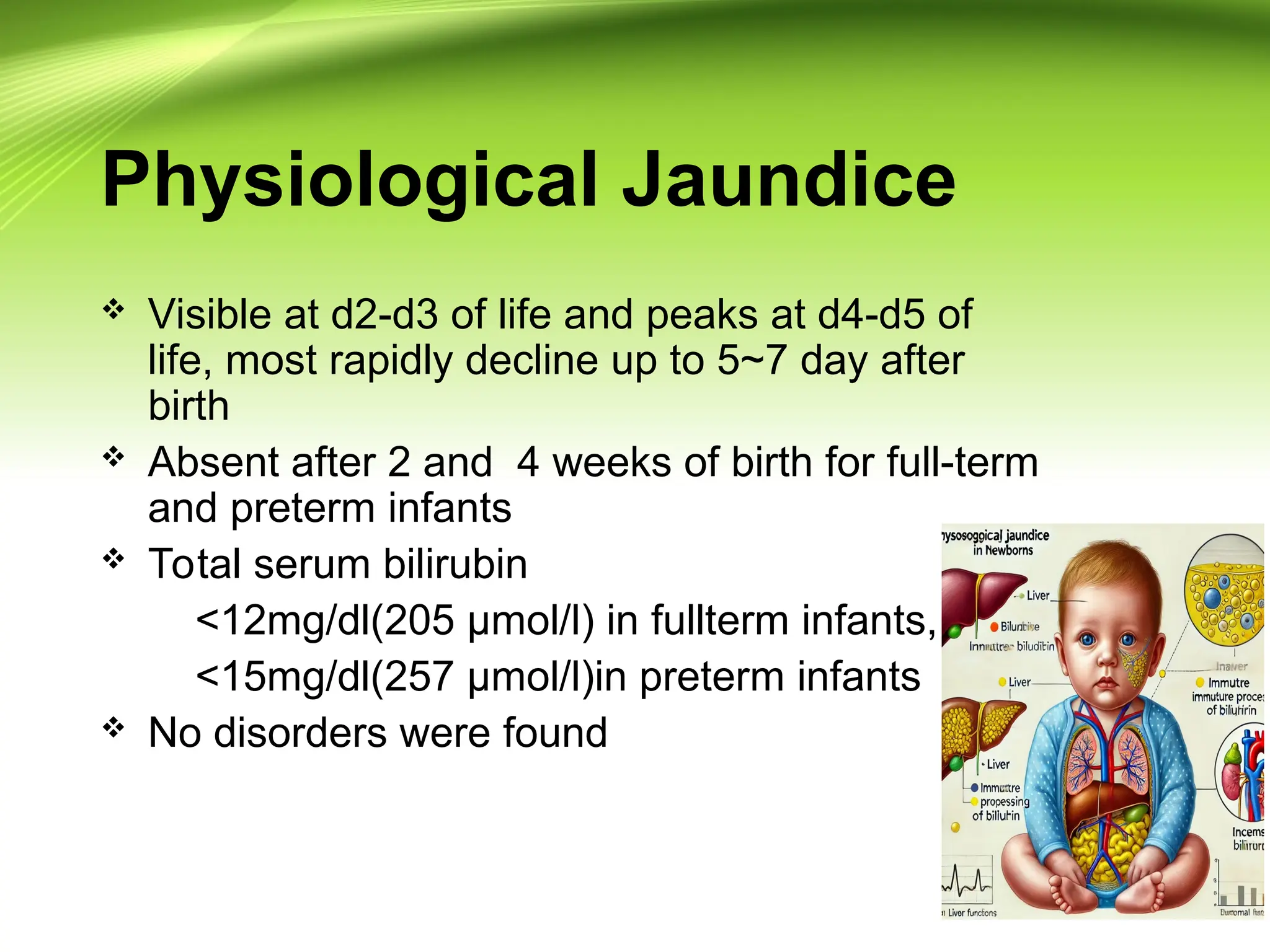
Physiological Jaundice
Visibleat d2-d3 of life and peaks at d4-d5 of
life, most rapidly decline up to 5~7 day after
birth
Absent after 2 and 4 weeks of birth for full-term
and preterm infants
Total serum bilirubin
<12mg/dl(205 µmol/l) in fullterm infants,
<15mg/dl(257 µmol/l)in preterm infants
No disorders were found
18.
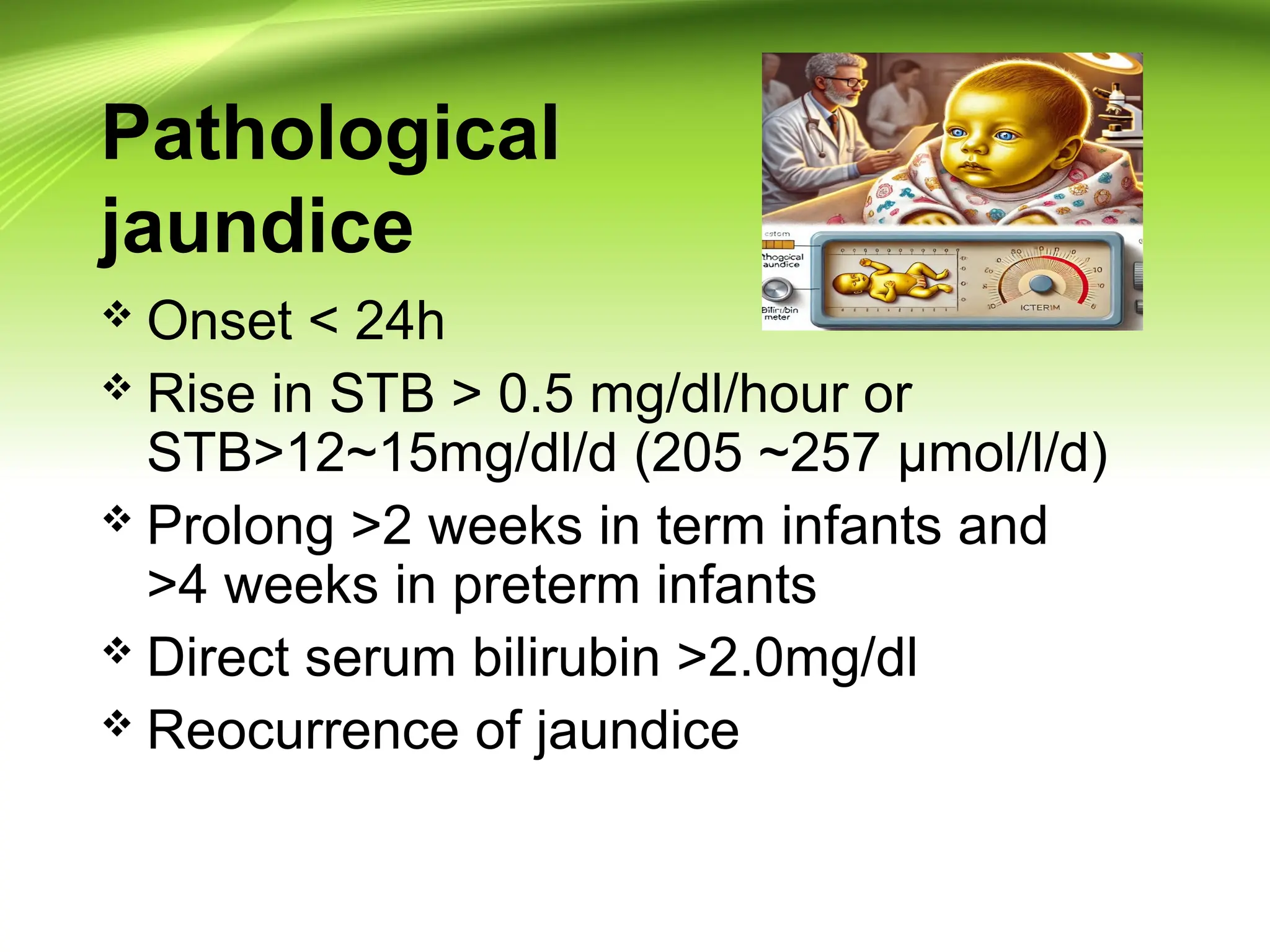
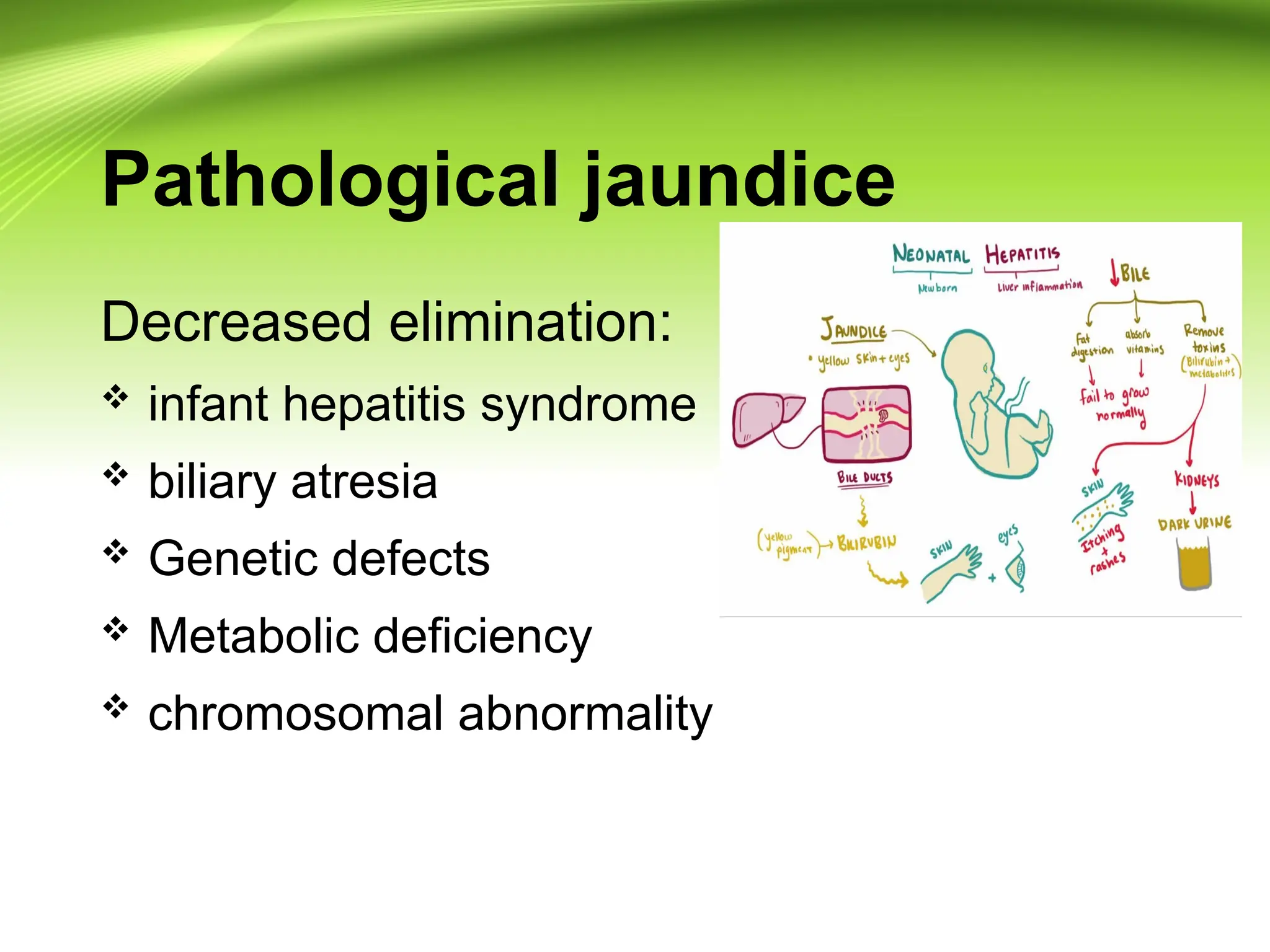
Pathological
jaundice
Onset <24h
Rise in STB > 0.5 mg/dl/hour or
STB>12~15mg/dl/d (205 ~257 µmol/l/d)
Prolong >2 weeks in term infants and
>4 weeks in preterm infants
Direct serum bilirubin >2.0mg/dl
Reocurrence of jaundice
Breastfeeding and Jaundice
•Breast milk jaundice Early onset
1. High bilirubin levels after 3 days of life
2. Related to a increased intake of milk
25.
Breastfeeding and Jaundice
•Breast-milk jaundice Late onset
1. High bilirubin levels by day 5-7 of life
2. Rise to peak level by 2 weeks of age
3. Bilirubin fall rapidly if stop breastfeeding
4. Rule out pathological condition
5. Mechanism is unknown(β-glucuronase)
Jaundice starting at<24 hrs of age
Hemolytic disorders
Rhesus incompatibility
ABO incompatibility
G6PD deficiency
Spherocytosis
Pyruvate kinase deficiency
Congenital infection
28.
Jaundice at 24hrsto 2 weeks of age
Physiological jaundice
Breast milk jaundice
Infection (UTI)
Bruising
Polycythemia
Crigler-Najjar syndrome
29.
Jaundice at >2weeksof age
Uncongugated
Physiological or Breast milk jaundice
Infection (UTI)
Hypothyroidism
Hemolytic anemia (G6PD deficiency)
High gastrointestinal obstruction (pyloric sten
osis)
Congugated
Bile duct obstruction
Neonatal hepatitis
Diagnosis
Blood test
bloodtype
reticulocyte count increases
Erythroblasts (also known as nucleated red
blood cells) occur
serum bilirubin levels may rise excessively ,most
is unconjugated bilirubin
32.
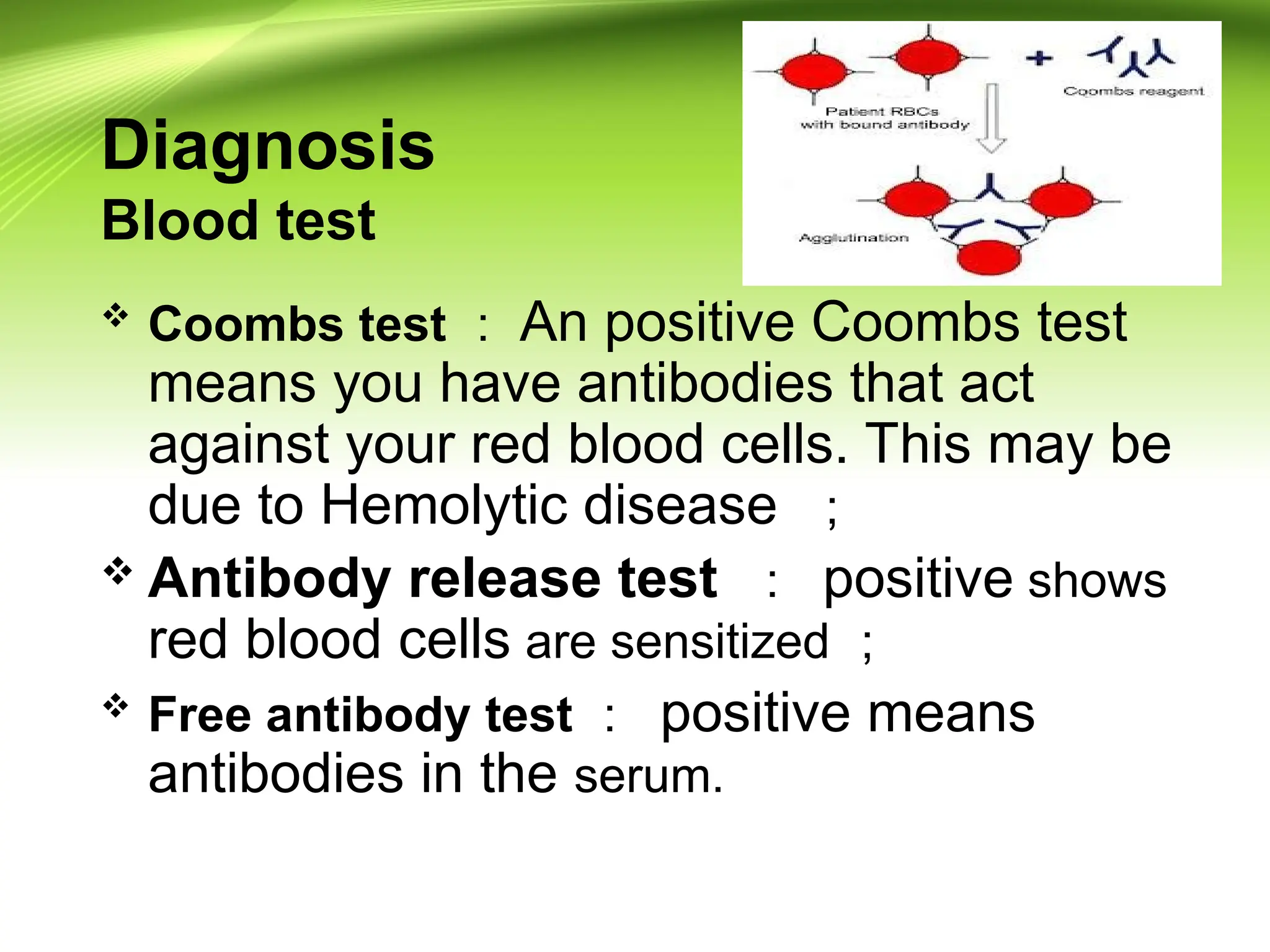
Diagnosis
Blood test
Coombstest : An positive Coombs test
means you have antibodies that act
against your red blood cells. This may be
due to Hemolytic disease ;
Antibody release test : positive shows
red blood cells are sensitized ;
Free antibody test : positive means
antibodies in the serum.
33.
Treatment
Treatment dependson the severity of the
condition, but could include phototherapy,
exchange transfusion with a blood
type compatible with both the infant and the
mother, sodium bicarbonate for correction
of acidosis and so on.
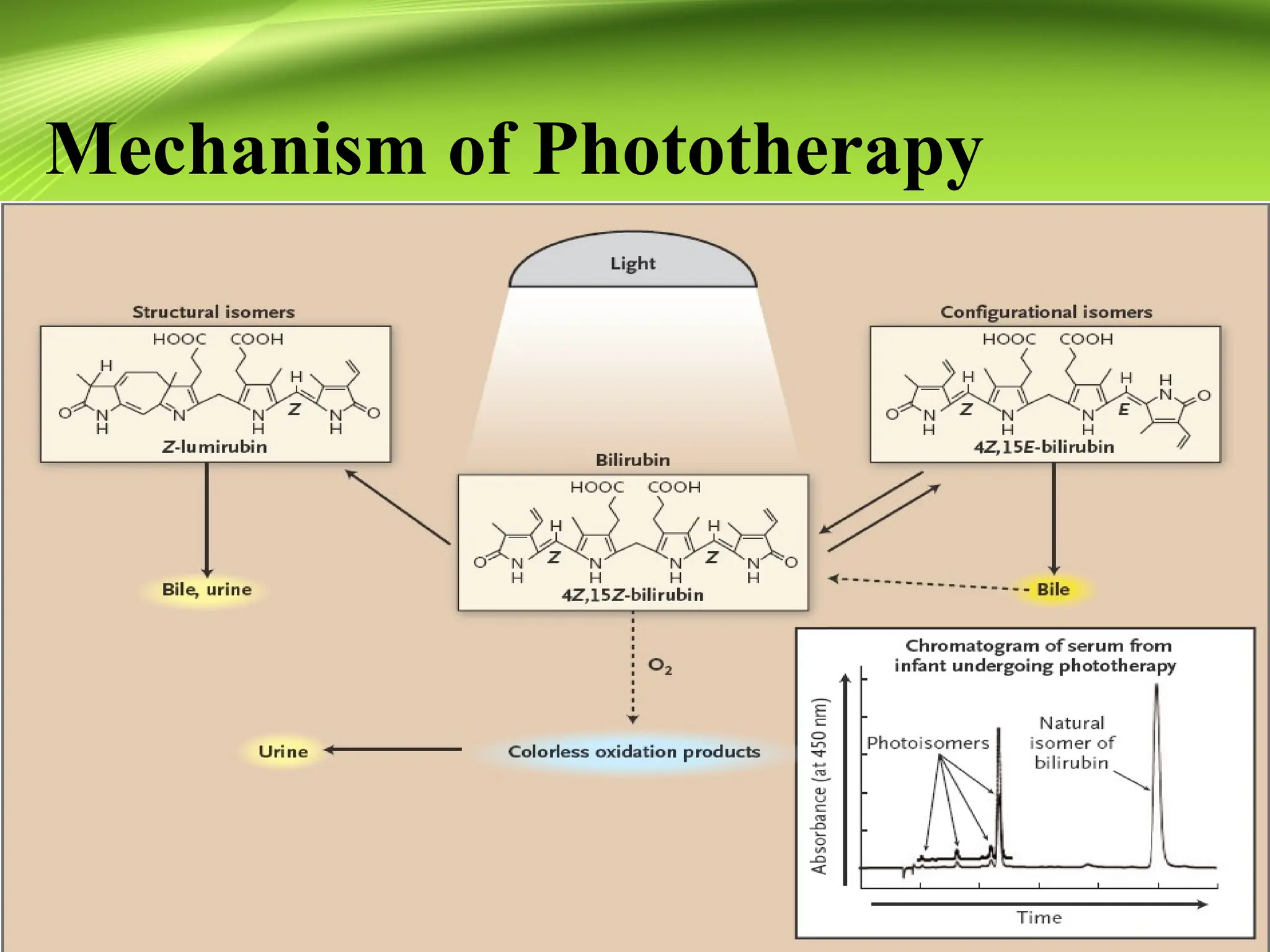
Treatment: Phototherapy
Effectiveand safe method of reducing
unconjugated hyperbilirubinemia
Blue-green light transforms bilirubin to
lumirubin, it is water soluble and excreted
in the urine
Drugs-IVIG
IVIG --- toreduce the need for exchange
transfusions.
The mechanism is related to blockage of Fc
receptors in the neonatal mononucler-macrophage
system.
Albumin--- to prevent bilirubin encephalopathy
Combine the unconjected bilirubin in the blood.
Indication of exchange
transfusion
Anemia (cord hemoglobin < 12 g/dL) , cord
bilirubin level (>68 µmol/L or 4 mg/dL), or enlarged
liver and/or spleen,generalized swelling,heart
failure.
Serum bilirubin level (>12 µmol/L /h or 0.7
mg/dL/h) ;
Serum bilirubin level >342µmol/L (20 mg/dL) or a
rate of increase that predicted this level or higher
Early symptoms of Bilirubin encephalopathy
41.
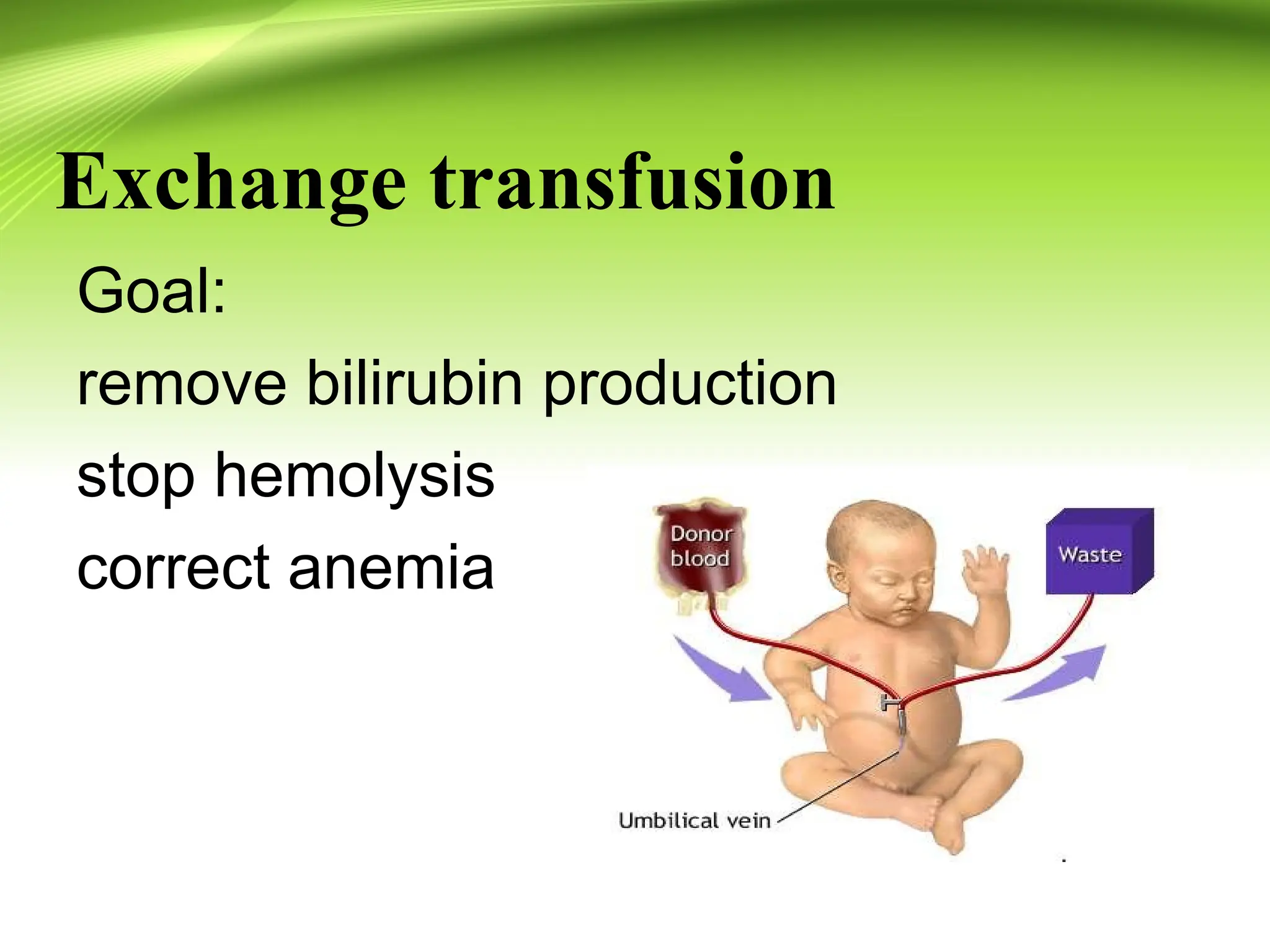
Exchange transfusion
(1) Indication
“IfTSB ≥25 mg/dl (428 μmol/l) or ≥20
mg/dl (342 μmol/l) in a sick infant or infant
<38 wk gestation, obtain a type and
crossmatch, and request blood in case an
exchange transfusion is
necessary”(Nelson Textbook of
Pediatrics, 18th edition)
(2) Mechanisms
Remove antibodies, antibody-coated RBCs
(sensitized red blood cells) and
bilirubin ,correct anemia
42.
Exchange transfusion
Blood
Rhhemolytic disease:Rh cross-matched against
the mother, ABO cross-matched against the
infant
ABO hemolytic disease: type O cells with AB
plasma
Volume
Double the volume of the infant’s blood (two-
volume exchange), 150-180ml/kg
Complications
Hypocalcemia, hypoglycemia, Acid-base
balance, hyperkalemia, embolization, bleeding,
infections