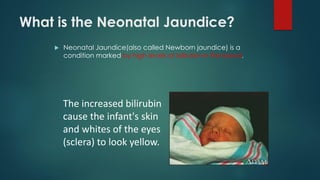
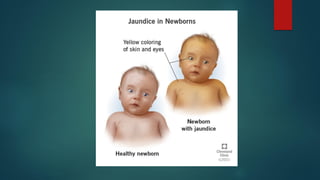
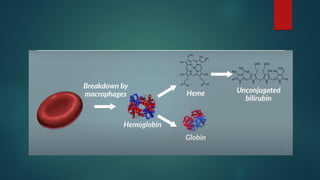
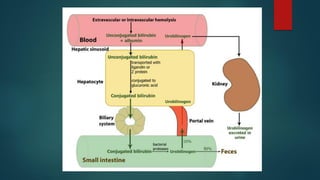
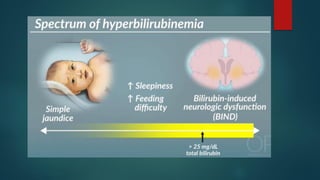
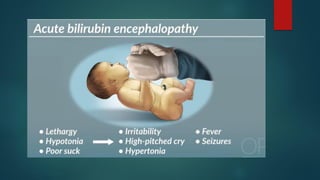
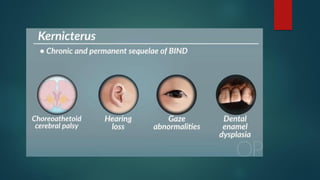
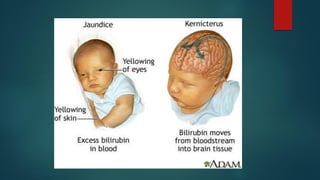
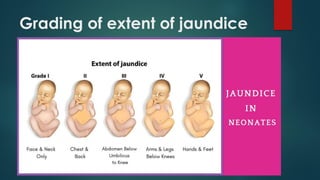
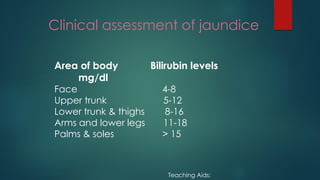
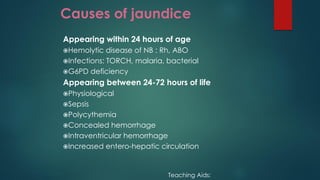
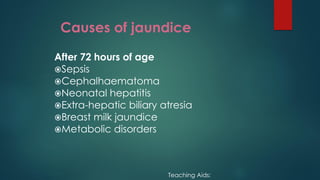
This document discusses neonatal jaundice (NJ), including what it is, common causes, how to identify it, potential complications, diagnostic tests, phototherapy treatment options and precautions, and types of phototherapy. NJ is a condition seen in many newborns marked by high bilirubin levels causing yellowing of the skin and eyes. It is usually benign and temporary but can become pathological if bilirubin levels get too high, requiring treatment like phototherapy or exchange transfusions to prevent complications like brain damage.