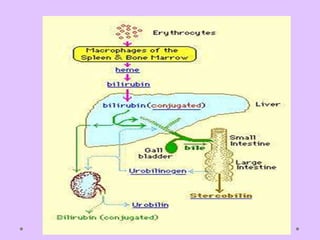
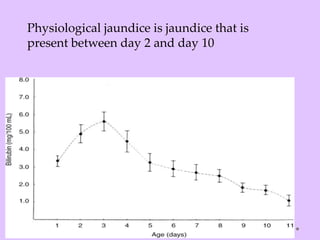
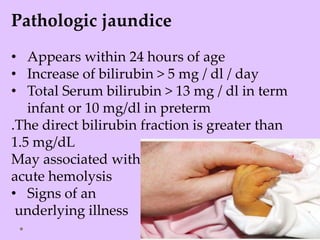
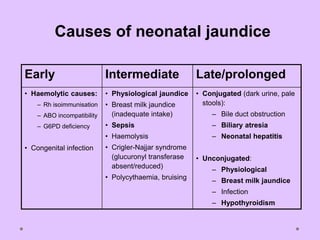
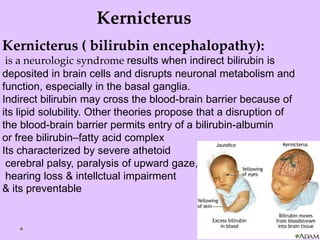
Physiologic jaundice is a common cause of hyperbilirubinemia in newborns resulting from increased bilirubin production, shortened RBC lifespan, and hepatic immaturity. It presents between 2-10 days of life with indirect bilirubin levels <12 mg/dL in term infants peaking on day 3. Kernicterus is a neurological syndrome caused by bilirubin deposition in the brain and can be prevented by avoiding excessively high indirect bilirubin levels >25 mg/dL. Diagnosis of hyperbilirubinemia involves history, physical exam, and laboratory tests including total, direct and indirect bilirubin levels as well as blood typing if levels are































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










