Downloaded 29 times





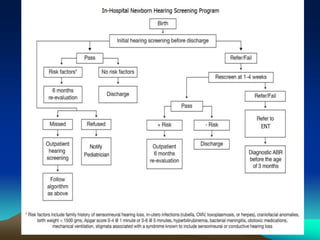


1. Newborn hearing screening allows for early detection of hearing loss, which is important as it can affect language development and social interactions. Screening tests like OAE and AABR that are inexpensive, portable and automated are used. 2. Risk factors for hearing loss include family history, neonatal intensive care, infections, syndromes etc. Any infant who does not pass the screening requires further evaluation. 3. Screening the newborns is crucial as it allows for early intervention if needed, which can improve speech and language outcomes. Pediatricians have an important role in ensuring all newborns receive and follow-up on screening.