Download to read offline


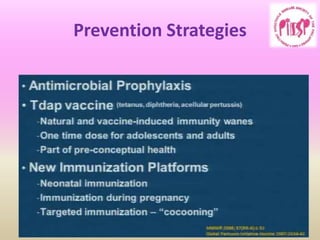
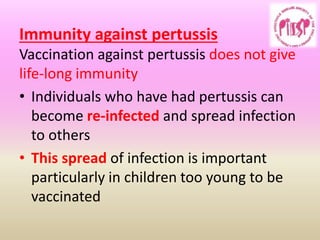

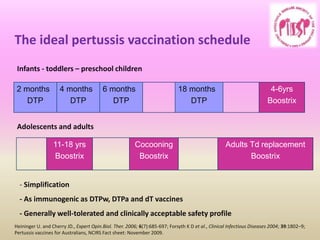



This document outlines pertussis (whooping cough), including why it continues to cause concern, epidemiology, clinical characteristics, diagnosis, complications, prevention strategies, and management of suspected cases. Pertussis is highly contagious and can cause severe illness in infants too young to be vaccinated. Vaccination of pregnant women is recommended to provide antibodies that protect newborns. While vaccination has reduced cases, pertussis remains a problem due to waning immunity over time. Improved vaccines and boosters are needed to better prevent the disease.





































![Pertussis in childhood._pediatrics_in_review_2012[1]](https://cdn.slidesharecdn.com/ss_thumbnails/pertussisinchildhood-170710084205-thumbnail.jpg?width=640&height=640&fit=bounds)






























![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


