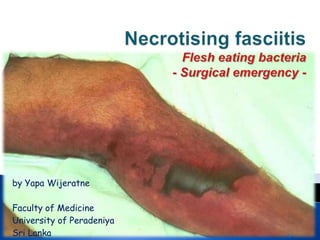
Necrotising fasciitis.by.Yapa Wijeratne
•Download as PPTX, PDF•
13 likes•8,184 views

Necrotising fasciitis is a surgical emergency having mortality 30–50% even with the best care. Therefore immediate diagnosis & management is a must.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Necrotising fasciitis.by.Yapa Wijeratne
Similar to Necrotising fasciitis.by.Yapa Wijeratne (20)
More from Yapa
More from Yapa (20)
Necrotising fasciitis.by.Yapa Wijeratne
- 1. by Yapa Wijeratne Faculty of Medicine University of Peradeniya Sri Lanka
- 2. Infection of subcutaneous tissue-> destruction of fascia and fat Rapidly progressive bacterial infection Pain, erythema edema, fever->severe pain with limb swelling->high fever, bluish discoloration & blisters Gangrene and & muscle necrosis
- 3. 1. Oedema beyond area of erythema 2. Crepitus 3. Skin blistering 4. Fever (often absent) 5. Greyish drainage (‘dishwater pus’) 6. Pink/orange skin staining 7. Focal skin gangrene (late sign) 8. Final shock, coagulopathy and multiorgan failure
- 5. Polymicrobial, synergistic infection – Most commonly a streptococcal species (group aβ haemolytic) in combination with Staphylococcus, Escherichia coli, Pseudomonas, Proteus, Bacteroides or Clostridium; 80% have a history of previous trauma/infection over 60% commence in the lower extremities.
- 6. 1. Diabetes 2. Smoking 3. Penetrating trauma 4. Pressure sores 5. Immunocompromised states 6. Intravenous drug abuse 7. Skin damage/infection (abrasions, bites & boils)
- 7. Febrile and tachycardic (early stages) Very rapid progression to septic shock. Oedema stretching beyond visible skin erythema, Disproportionate pain in relation to the affected area Skin vesicles Palpation ◦ A woody hard texture to the subcutaneous tissues, ◦ An inability to distinguish fascial planes & muscle groups ◦ Soft-tissue crepitus. Lymphangitis tends to be absent.
- 8. Radiographs : air in the tissues Diagnosis: on the basis of symptoms and signs without recourse to ‘screening radiography’ unnecessary delay may be lethal.
- 9. 1. Urgent fluid resuscitation, 2. Monitoring of haemodynamic status 3. High-dose broad-spectrum IV antibiotics. 4. Surgical debridement- diseased area should be debrided ASAP until viable, healthy, bleeding tissue is reached.
- 10. Advisable, ◦ Early review in the operating theatre ◦ Further debridement ◦ Use vacuum-assisted dressings. Early skin grafting - may minimise protein and fluid losses. Mortality 30–50%
- 11. Case 76 yr old H/w from Kandy presented with swelling of the left LL for 5days. She was apparently well before & developed mild fever with left leg pain. Leg pain was severe, resting type, not radiating, persistent throughout the day, & not responding to the PCM. Swelling was developed with redness & accidental trauma has ulcerated the causing discharge. She was admitted to the local hospital on 3rd day but no surgical intervention was made. 5th day after onset of symptoms she was transferred to THK. She has had STEMI 1yr ago. No Diabetes mellitus. On admission she was afebrile, haemodynamically stable. Examination of CVS, RS, abdomen & NS clinically normal. WBC 29k/ul ↑↑ Urea 125 mg/dl (10-50) ↑↑ SE, RBC, Hb, PLT, RBS normal. ECG: sinus arrythmia, p mitrale ECHO revealed EF 45% impaired LV function with diastolic dysfunction. G II MR+ AR+
- 12. Spinal anesthesia given. Indurated upto mid thigh. Able to move toes. Skin necrosis +. Pulse – difficult to feel. Necrotized tissue excised. Underlying fascia split. Underlying muscle viable. Necrotising fasciitis
- 13. 1. NBM 2. QHT 3. Input/ output chart 4. Elevate footend 5. > 3 ʘ N/s IV 6. 2 ʘ Hartmann 7. IV meropenem 500mg bd 8. Tramadol 50 mg tds 9. Domperidone 10mg bd 10. IM Pethidine 75 mg SOS 11. IM Phenagan 25 mg SOS 12. Monitor PR/ RR/ BP 1 hrly