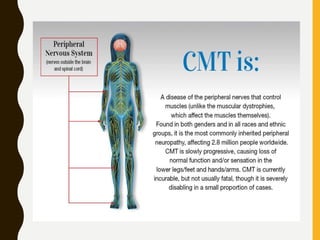
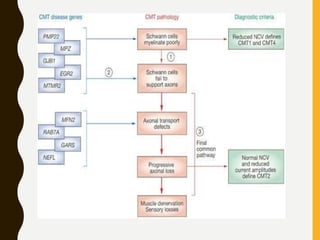
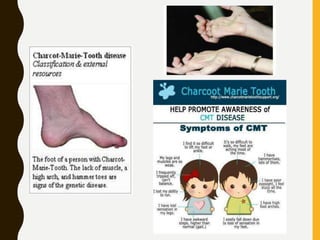
Charcot-Marie-Tooth disease (CMT) is a group of inherited neurological disorders that damage the peripheral nerves, causing muscle weakness, loss of sensation in the feet and hands, and deformities. CMT is caused by genetic mutations that affect the myelin sheath or axons in the nerves. There are several types of CMT including CMT1, CMT2, CMT4 and CMTX, which are distinguished by their genetic causes and symptoms. Currently there is no cure for CMT but treatment focuses on managing symptoms through physical therapy, bracing, and surgery. Researchers are investigating potential new treatments to help prevent disability and progression of the disease.


























































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)









