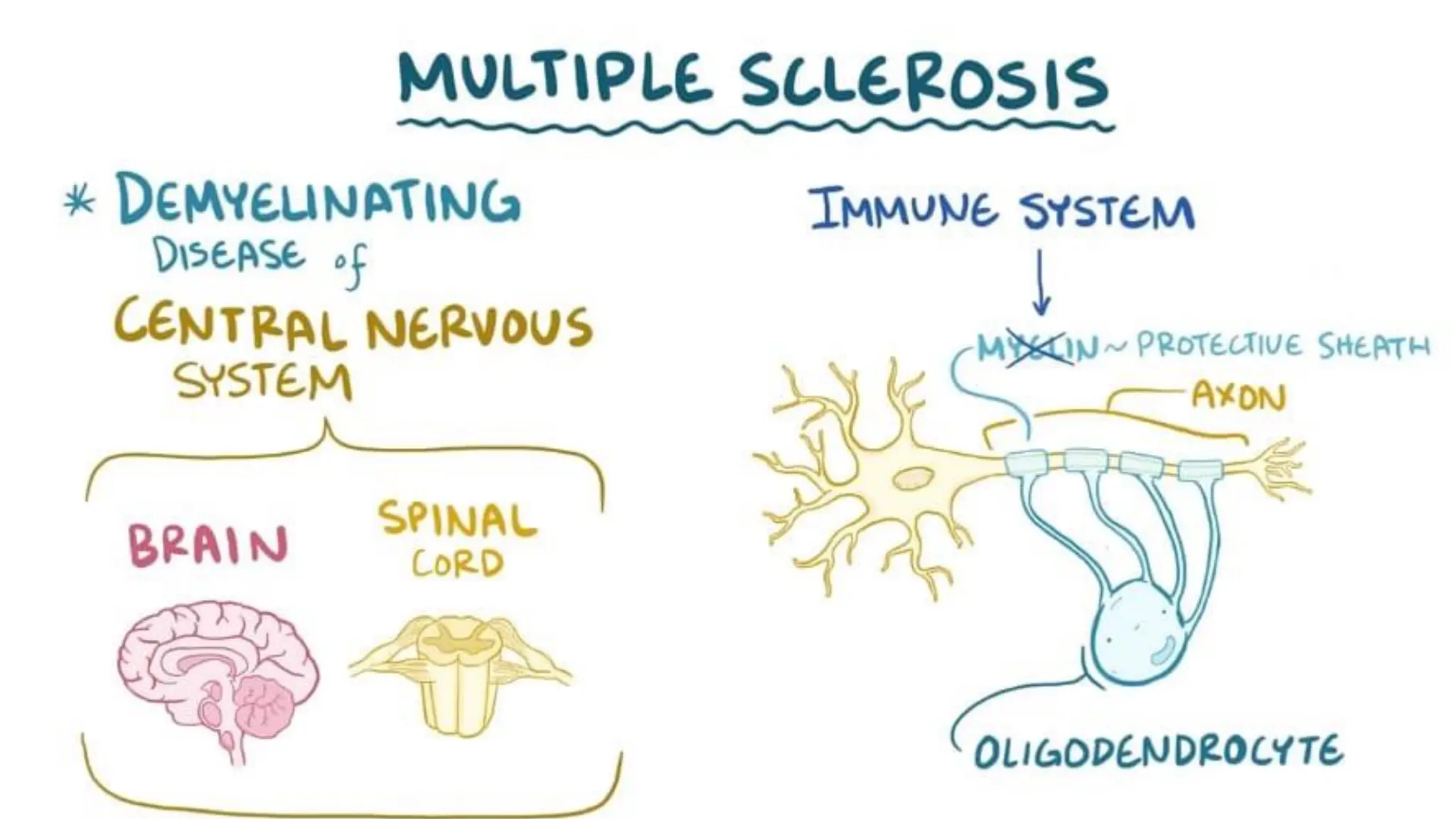
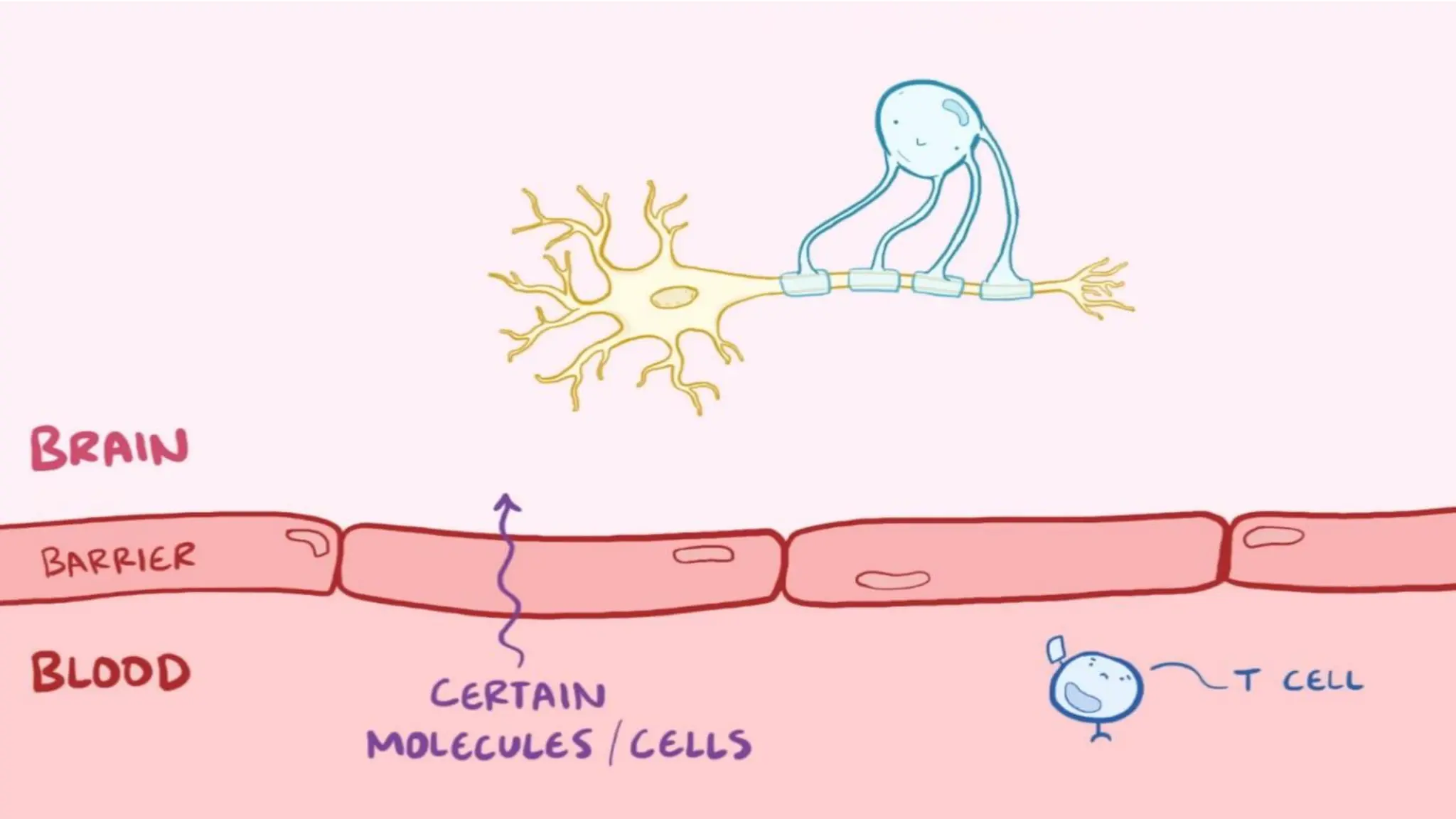
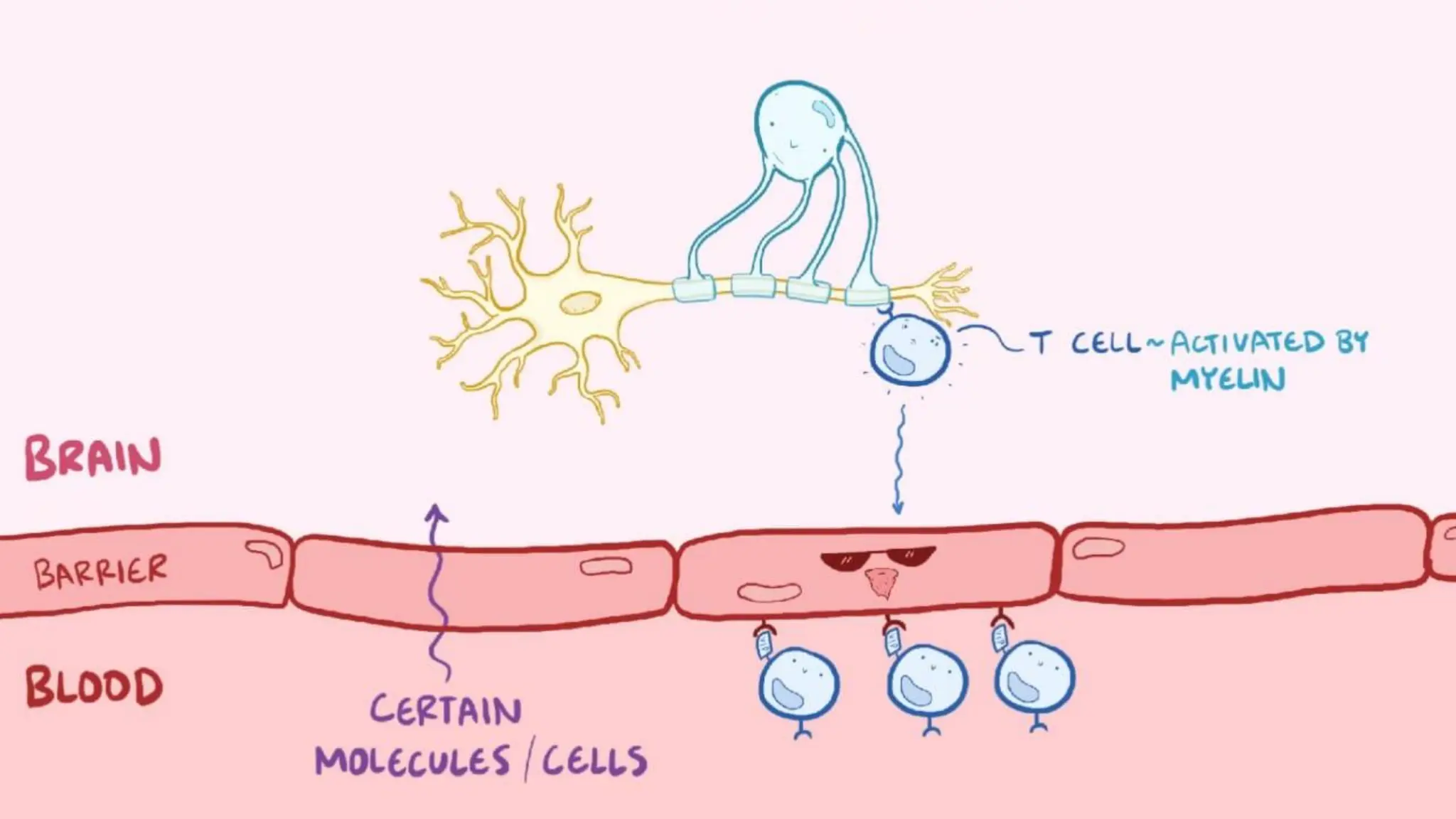
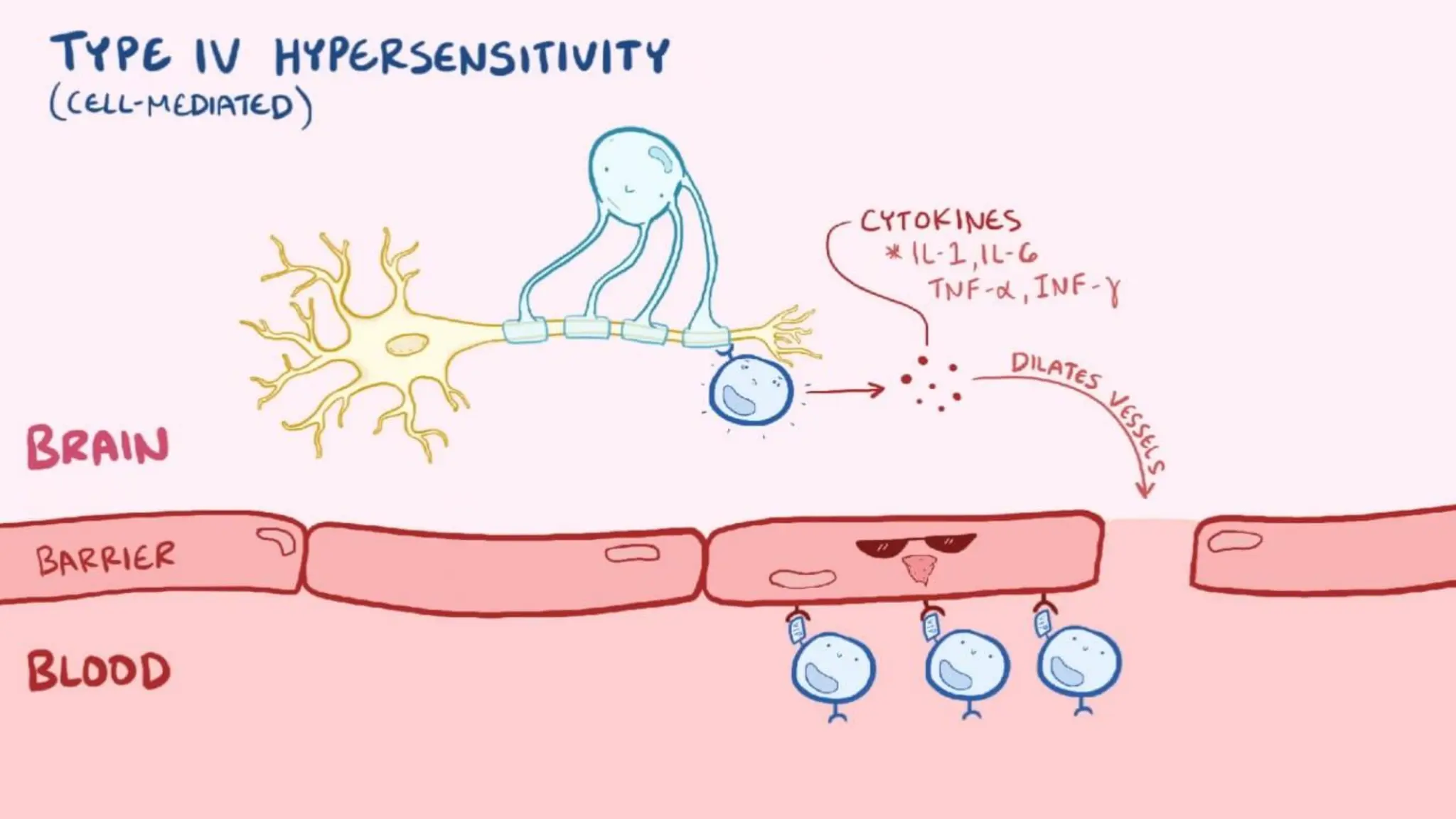
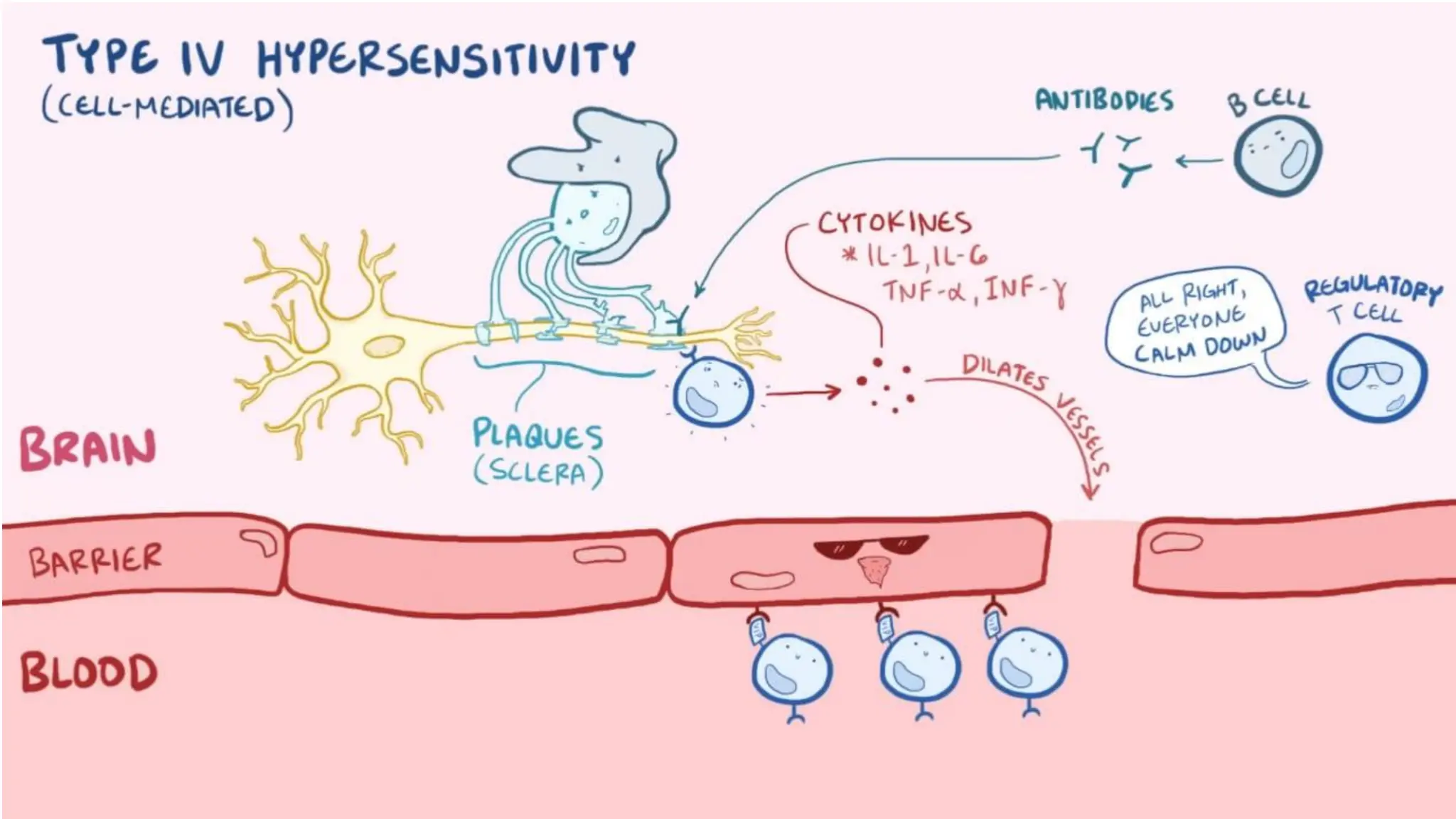
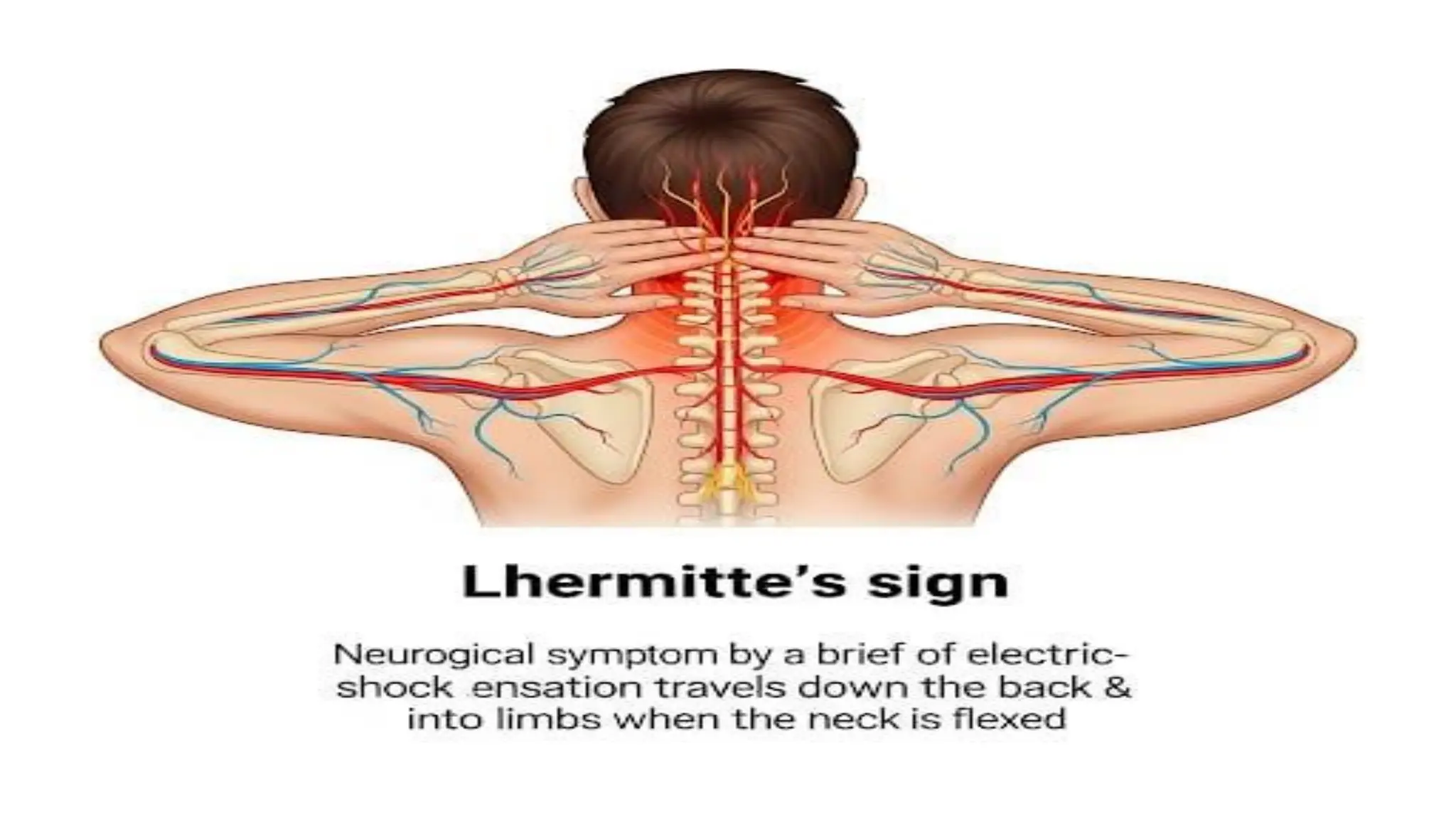
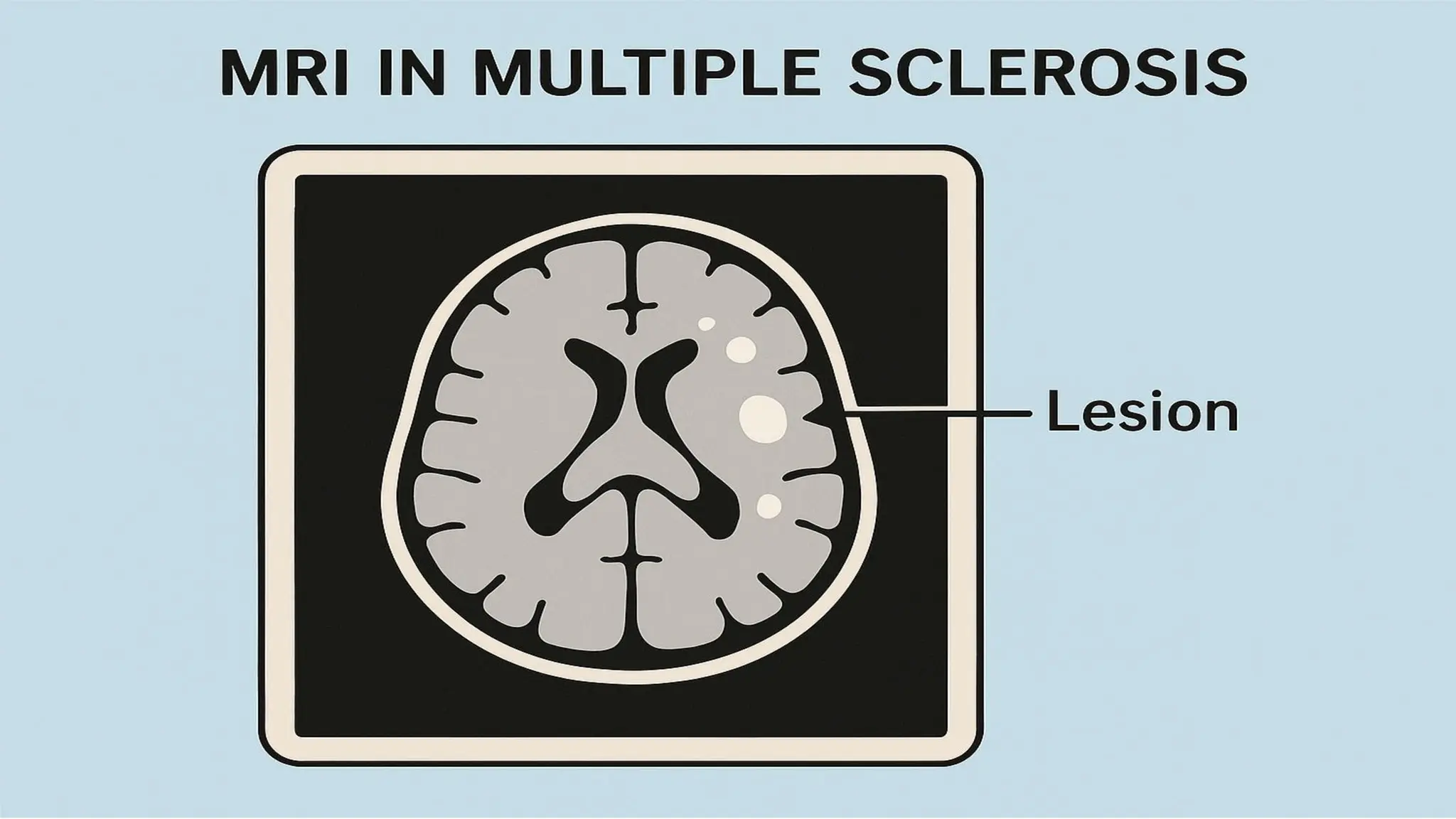
DEFINE Multiple sclerosis(MS)
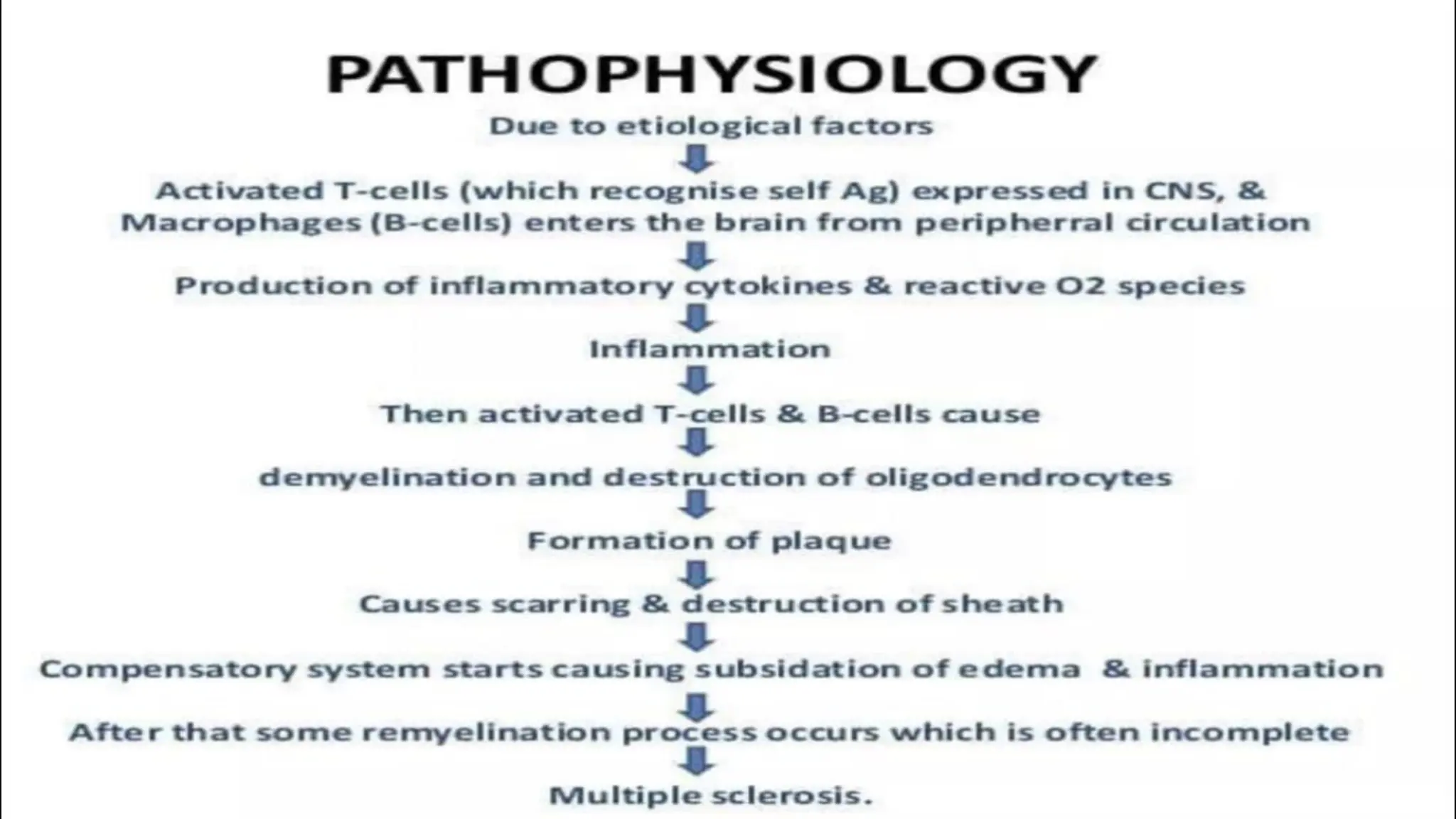
is an autoimmune
disease affecting the
central nervous system,
causing nerve damage,
impaired movement,
vision issues, and
cognitive difficulties.
9.
INCIDENCE
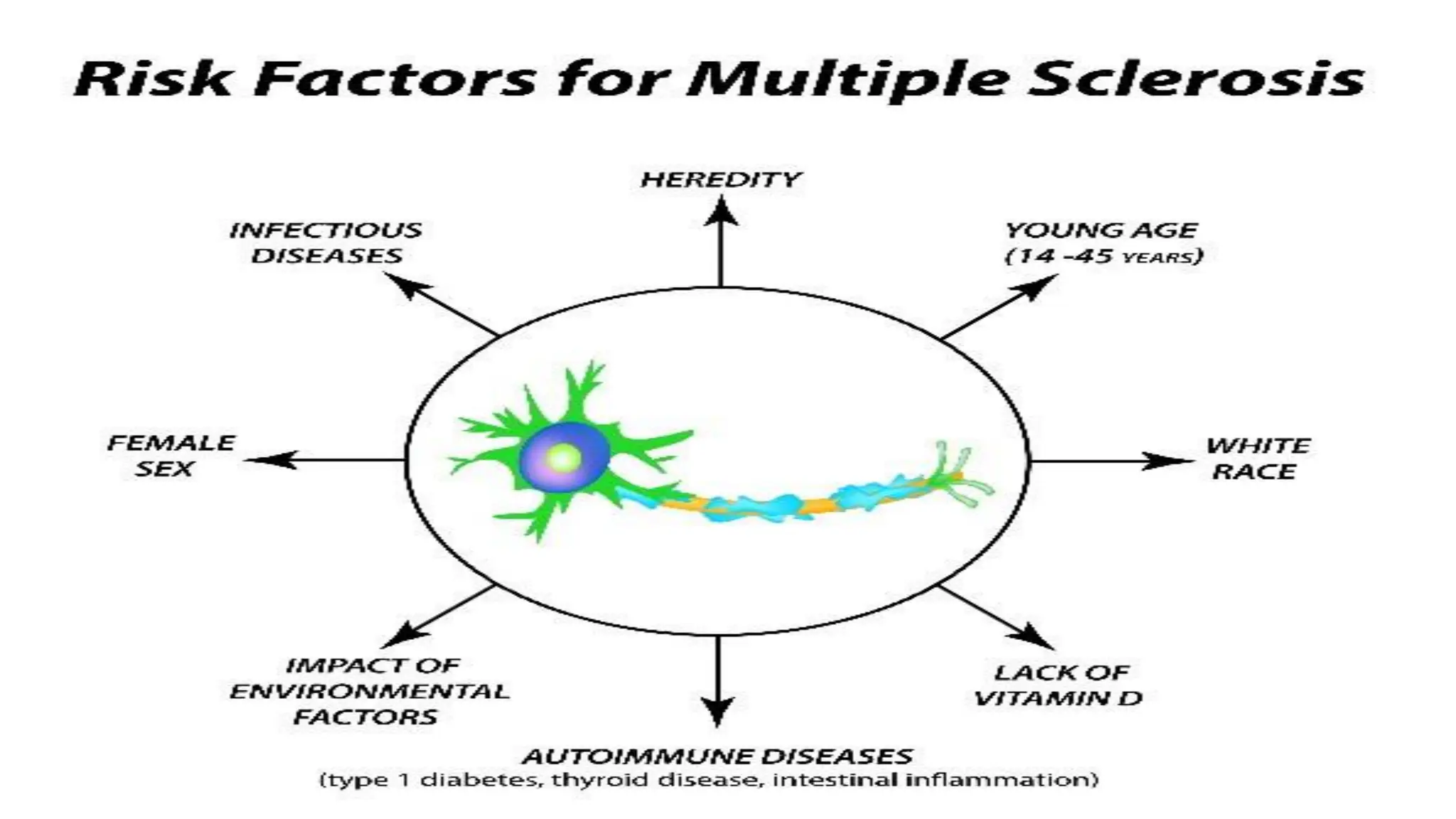
•Multiple sclerosis inwomen is 2-3
times more prevalent that in men
•It is not contagious
•Worldwide :- 1.1-2.5 million
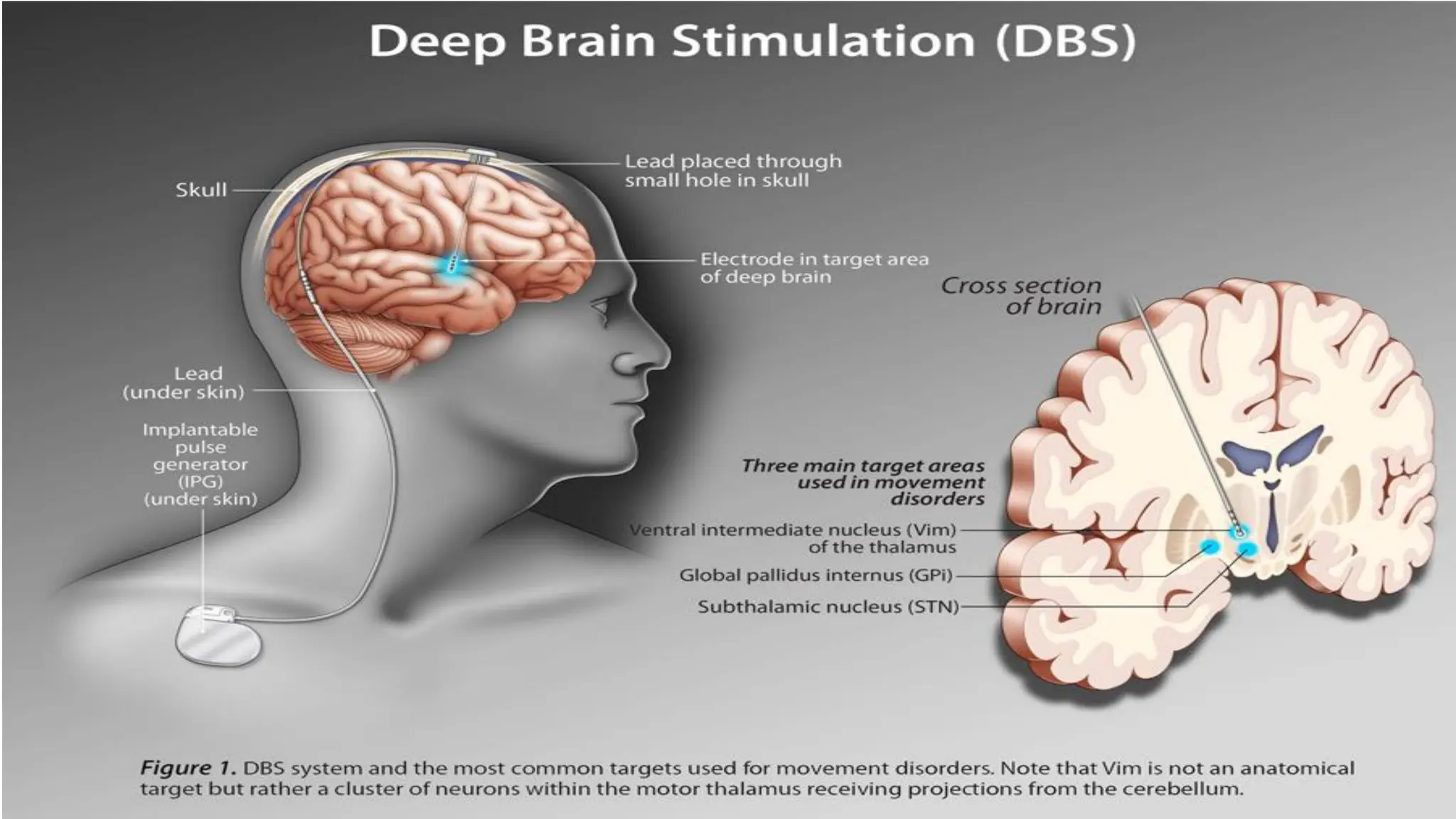
•DBS is aninvasive surgical procedure where
electrodes are permanently implanted into
specific deep brain regions, most commonly the
thalamus. These electrodes are connected by
wires to a small battery-powered device
(neurostimulator or "brain pacemaker")
implanted under the skin, usually near the
collarbone. The device sends continuous
electrical impulses to the brain, which helps to
block or regulate abnormal nerve signals.
53.
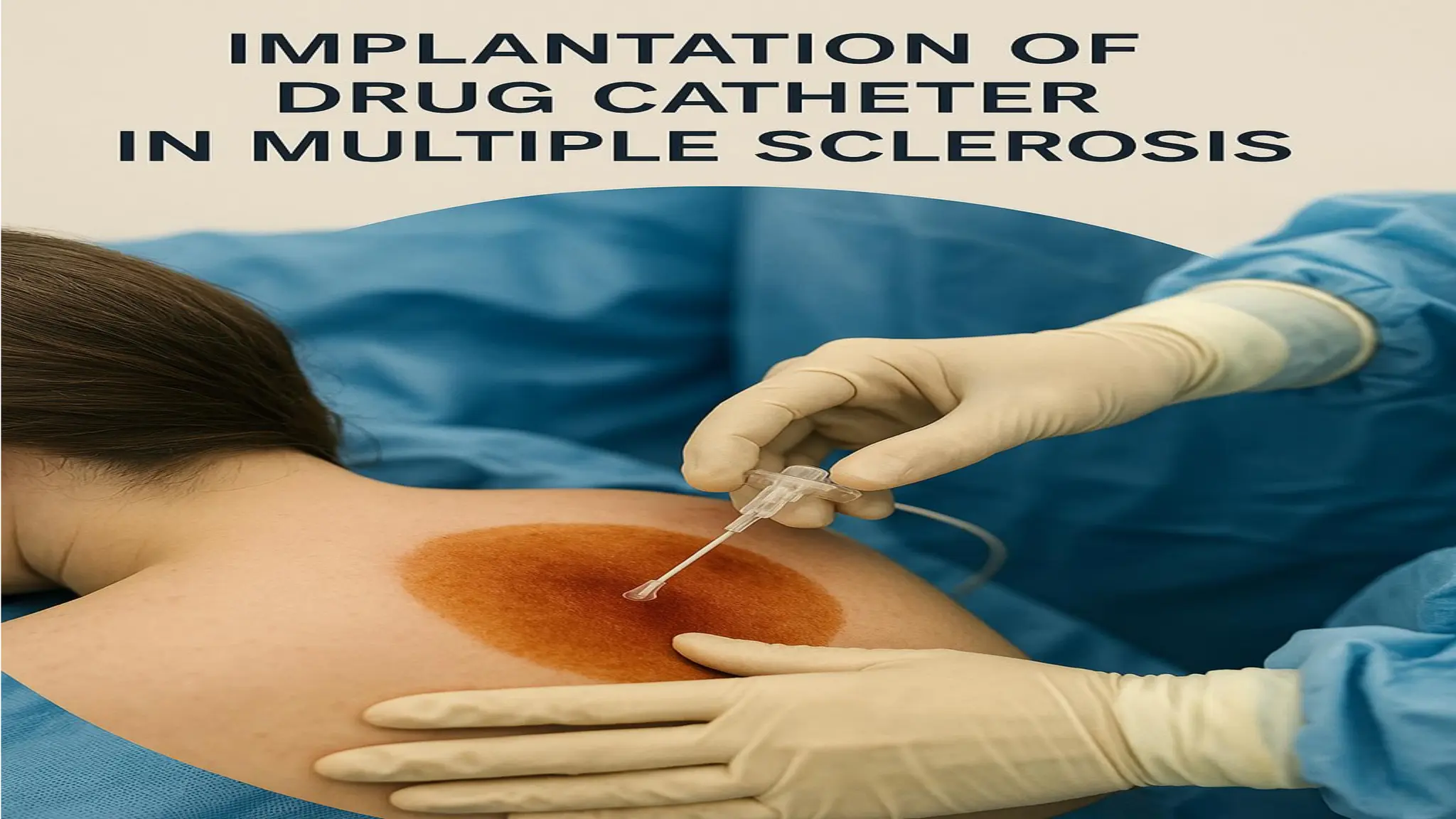
•Implantation of adrug catheter in multiple
sclerosis typically involves placing a catheter into
the spinal fluid (intrathecal space). This allows for
direct delivery of medications, such as baclofen
for severe spasticity, bypassing the blood-brain
barrier and minimizing systemic side effects. It's
often used for symptom management when oral
therapies are ineffective.
Chronic Pain relatedto nerve damage
(neuropathic pain), muscle spasm as
evidenced by patient report of pain
1. Assess the general condition
2. Provide hot and cold application
3. Position the patient comfortably
4. Administer Analgesics
5. Provide Emotional Support
56.
Impaired physical mobilityrelated to
muscle weakness as evidenced by
difficulty in performing ADL
1. Assess the general condition
2. Provide comfortable position
3. Assist the patient in performing ADL
4. Assist the patient in ambulation
5. Ensure safety precautions
57.
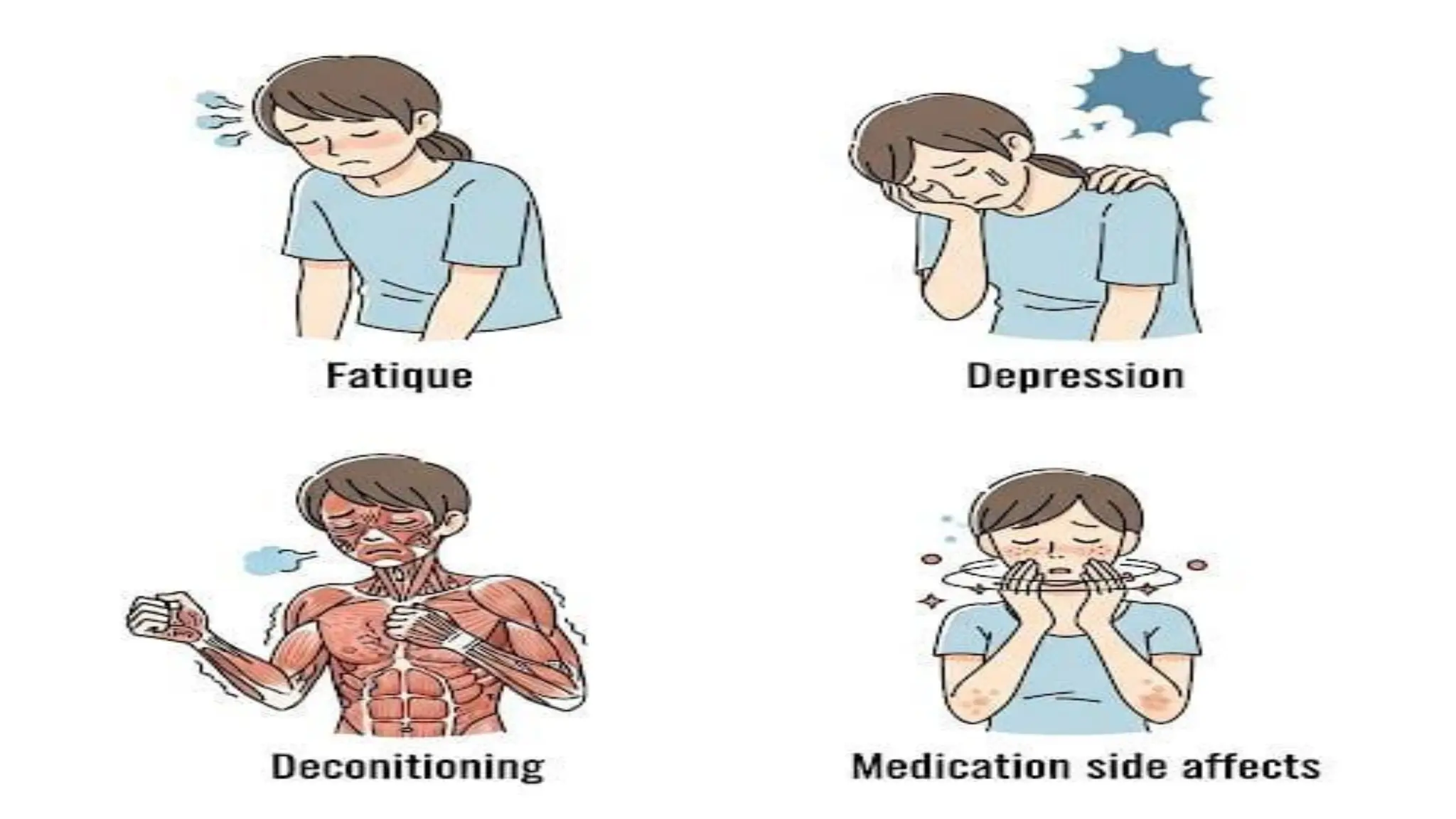
Fatigue related toincreased energy need as
evidenced by facial expression of client
1. Assess the general condition
2. Teach the patient about energy conserving
techniques
3. Encourage the patient to perform passive ROM
4. Promote sleep hygiene
58.
Risk for injuryrelated to impaired balance
and muscle weakness
1. Assess the general condition of the patient
2. Provide comfort devices to the patient
3. Assist the patient in ambulation
4. Educate the patient about assistive devices
59.
Risk for adultfall related to neurological
impairment
1. Assess the general condition of the patient
2. Raise the side rails of patient bed
3. Provide comfort devices
4. Assist the patient in ambulation
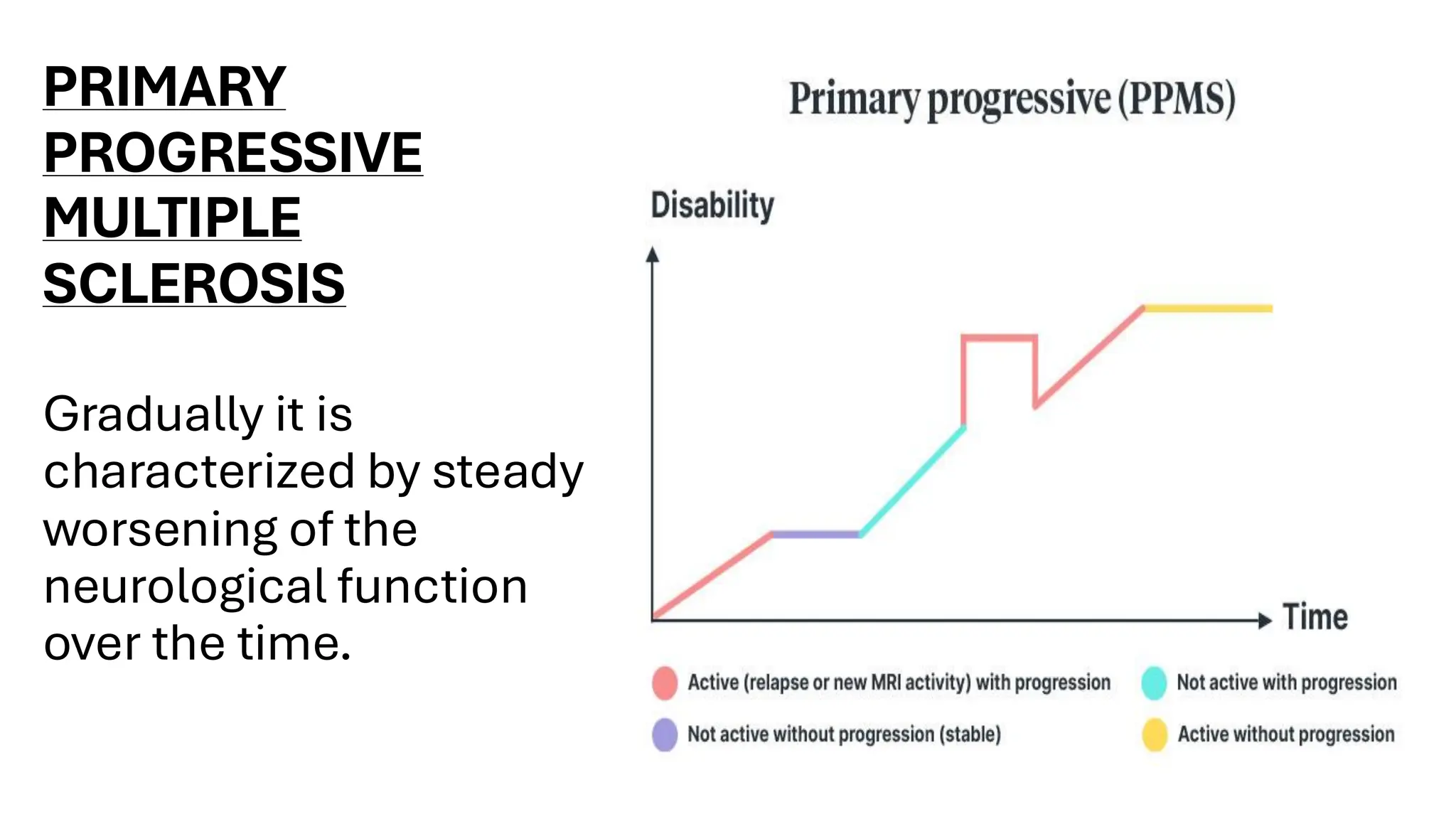
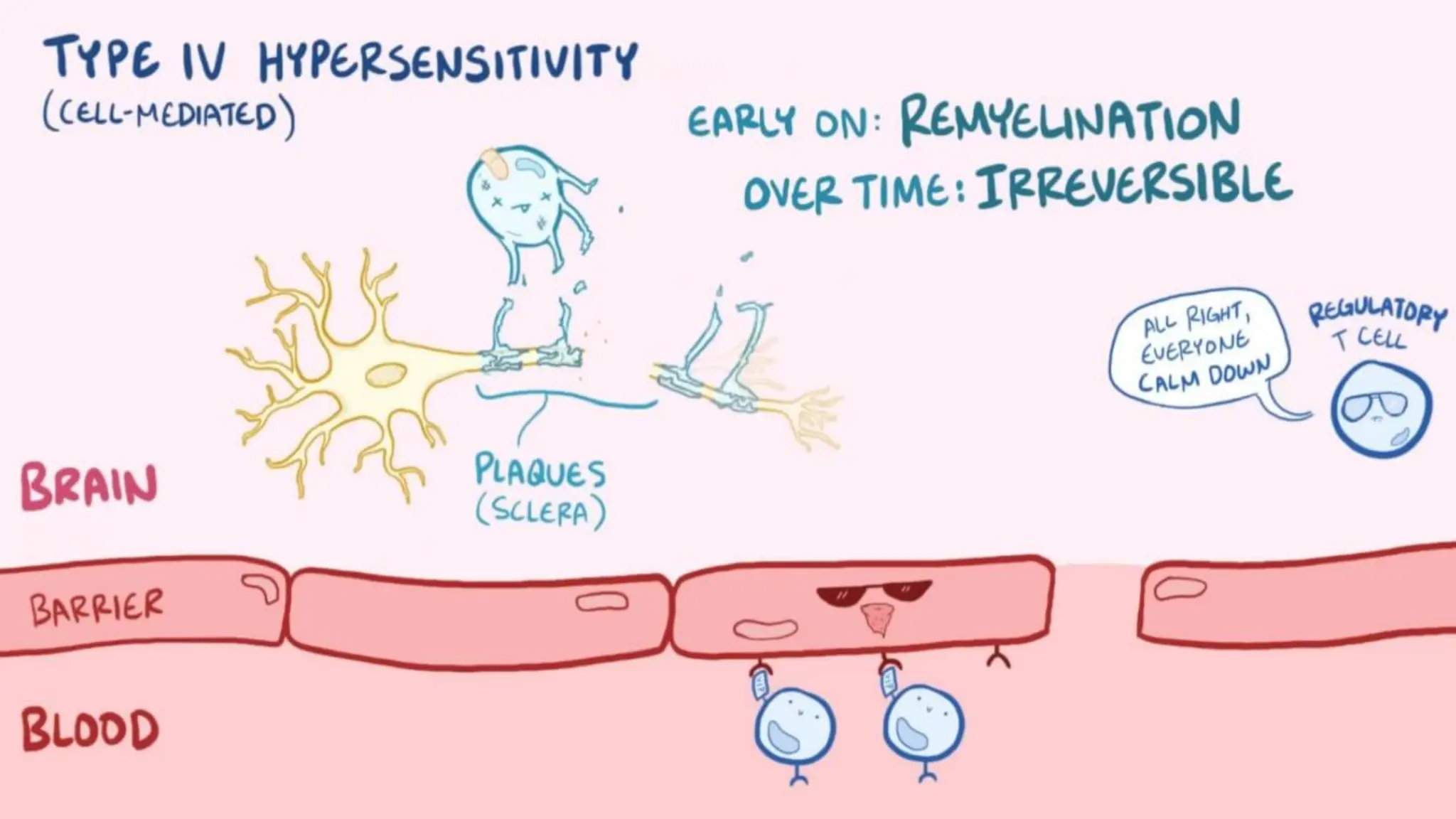
Multiple sclerosis isa
progressive autoimmune
disease affecting the
nervous system. Though
incurable, early diagnosis,
disease-modifying
therapies, and symptom
management improve
quality of life. Ongoing
research offers hope for
better treatments and
potential cures.
69.
BIBLOGRAPHY
▪GERARD TORTORA; BRYANDERRICKSON. PRINCIPLES OF
ANATOMY AND PHYSIOLOGY. 14th EDITION. PAGE NO. 332-
350
▪USHA UKANDE, JAIDEEP HERBERT,SHWETA PATTNAIK, ANIL
SHARMA. TEXTBOOK OF ADULT HEALTH NURSING. 2nd
EDITION.PAGE NO. 408-415
▪MJ KUMARI. ADULT HEALTH NURSING-I. 3rd EDITION. PAGE
NO. 205-218
▪JAVED ANSARI, DAVINDER KAUR. PEE VEE. TEXTBOOK OF
ADULT HEALTH NURSING. 4th EDITION. PAGE NO. 303-316