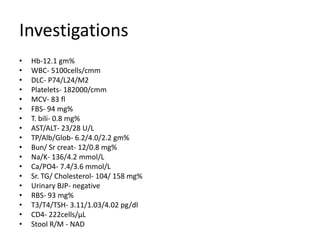
This case presentation describes a 42-year-old man who presented with progressive weakness, spasticity, and pseudobulbar palsy in his upper and lower limbs over the past 6 months. Clinical examination revealed features of both upper and lower motor neuron involvement. Investigations including MRI, CSF analysis, and EMG were consistent with a diagnosis of motor neuron disease. The patient was found to be HIV positive. Given his clinical presentation and HIV status, he was diagnosed with HIV-associated generalized motor neuron disease. The pathogenesis of motor neuron disease in the context of HIV is not fully understood but may involve retroviral myelopathy or reactivation of endogenous retroviruses. Treatment involves continuation of HAART and supportive measures





























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




