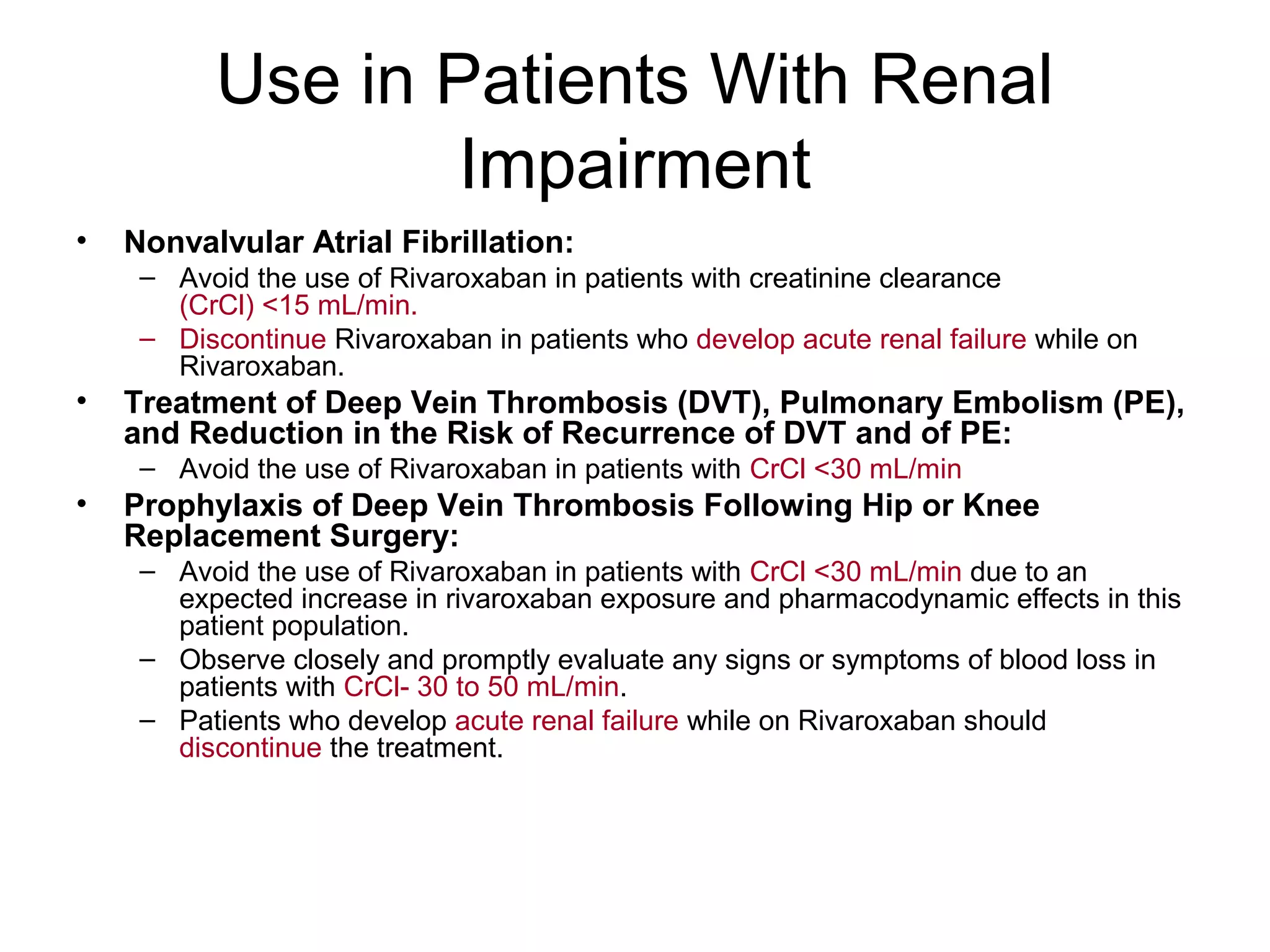
Rivaroxaban (Xarelto) is an oral anticoagulant that inhibits factor Xa and offers predictable therapeutic effects without the need for monitoring, making it preferable over traditional anticoagulants. It is indicated for various conditions, including reducing stroke risk in nonvalvular atrial fibrillation, treatment of DVT and PE, and prophylaxis after knee or hip replacement surgery. However, it has limitations, such as contraindications in patients with renal impairment below certain thresholds and the absence of a specific antidote for overdose.