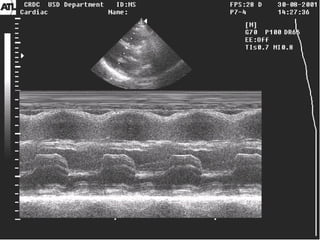
Downloaded 38 times

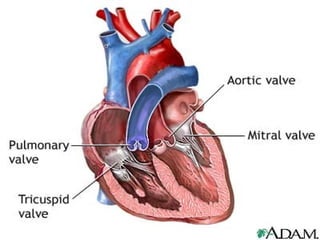
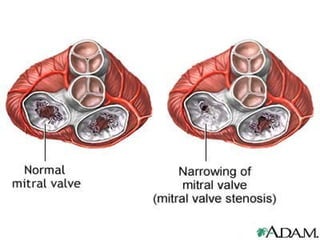




Mitral stenosis is a narrowing of the mitral valve opening that causes blood to back up in the lungs. It is usually caused by rheumatic fever which causes the mitral valve flaps to stick together. The main symptoms are shortness of breath, fatigue, and coughing. On examination, doctors may hear murmurs and find an enlarged heart and liver. Echocardiograms and chest x-rays can confirm the diagnosis by showing the narrowed valve opening and enlarged chambers. Treatment options include medications, balloon valvuloplasty to widen the valve, or open heart surgery to replace or repair the valve.























































































