This document provides information about microscopic examination of urine sediments. It describes how to prepare and examine urine samples under a microscope. Key points include:
- Centrifuging a urine sample to concentrate the sediment, then examining a drop under the microscope using both low and high power fields.
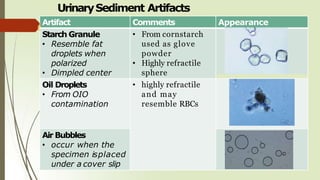
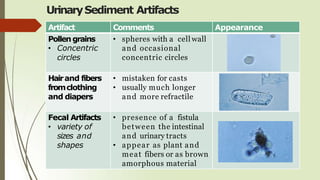
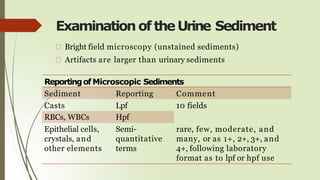
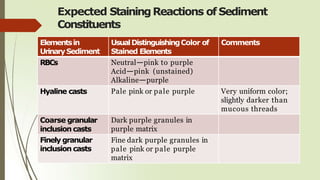
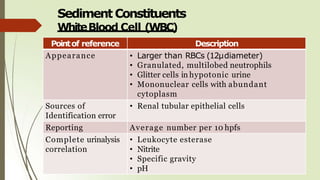
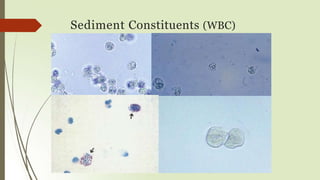
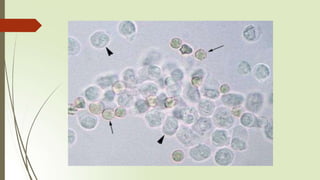
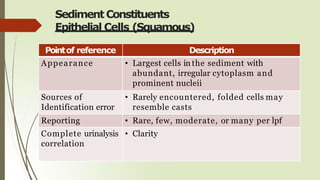
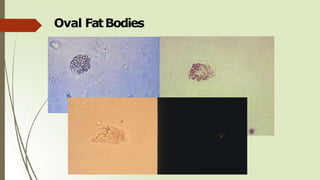
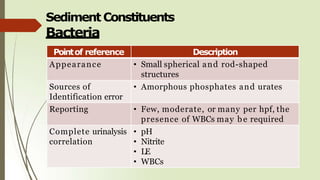
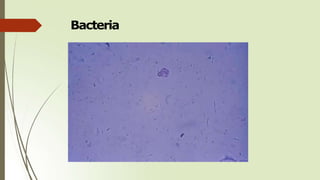
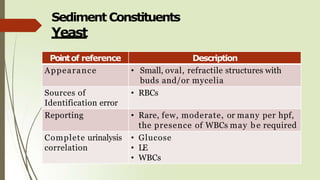
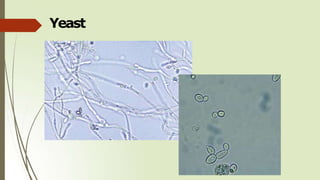
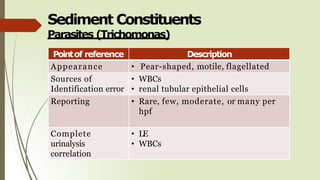
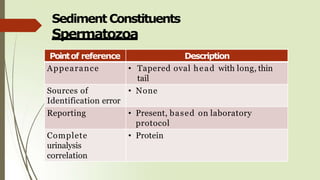
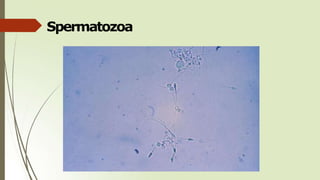
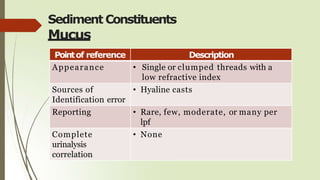
- Common elements found in urine sediments include red and white blood cells, epithelial cells, casts, crystals, bacteria, yeast, parasites, mucus, fat and other elements.
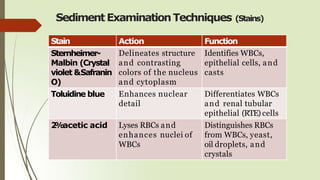
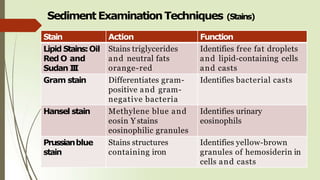
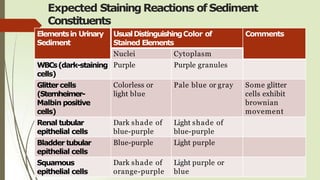
- Additional staining techniques can aid in identification, such as using Sternheimer-Malbin to identify white blood cells and epithelial cells.
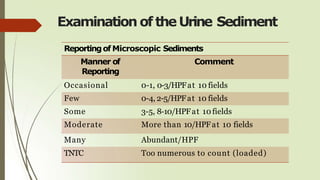
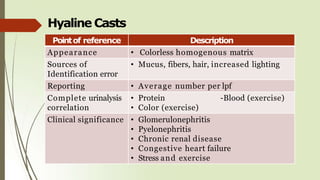
- Findings should be reported semi-quantitatively as rare, few, moderate or many.
-
![Examination oftheUrine Sediment
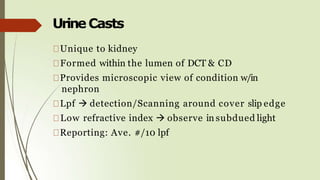
Observe minimum of 10 fields [both low & high PF]
LPF (10x)
detect casts and to ascertain the general
composition of the sediment
HPF (40x)
Identification
casts have a tendency to locate near the edges of
the cover slip (LPFscanning around the cover slip
perimeter)](https://image.slidesharecdn.com/microscopicexaminationofurinepdf1-230322023725-5582d6da/85/Microscopic_Examination_of_Urine_pdf-1-pptx-3-320.jpg)












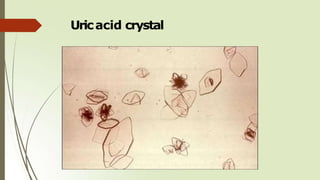
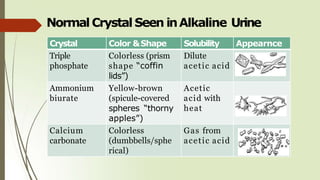
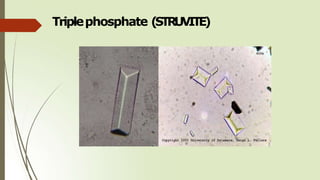
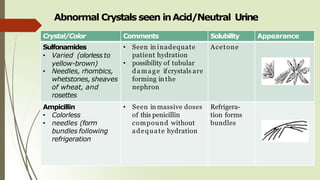
![Normal Crystal Seen inAcidic Urine
Crystal Color &Shape Solubility Appearnce
Uric Acid Yellow-brown
(rhombic/4-
sided/rosette)
Alkali
Soluble
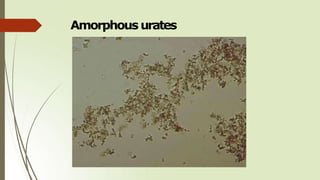
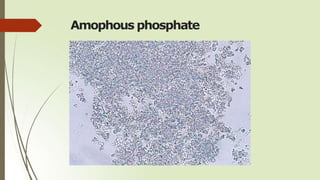
Amorphous
urates
Brick dust or
yellow brown
granules
Alkali and
heat
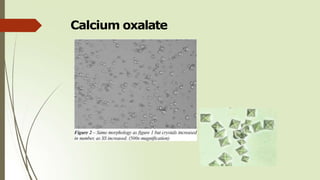
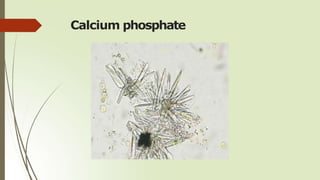
Calcium
oxalate
[Acid/neutral
(alkaline)]
Colorless
(envelopes, oval,
dumbbell,
octahedral)
Dilute HCl](https://image.slidesharecdn.com/microscopicexaminationofurinepdf1-230322023725-5582d6da/85/Microscopic_Examination_of_Urine_pdf-1-pptx-60-320.jpg)