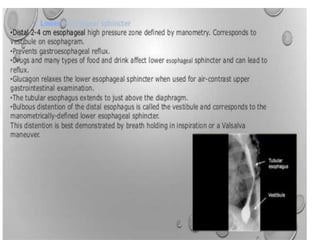
This document provides information about barium swallow studies, including:
- The learning objectives which are to describe the anatomy and physiology of the esophagus and the procedure for barium swallow studies.
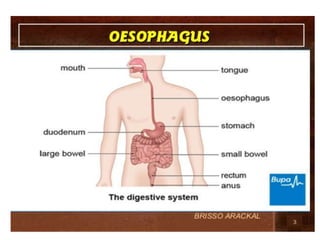
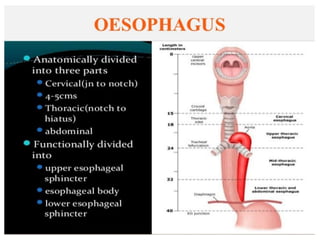
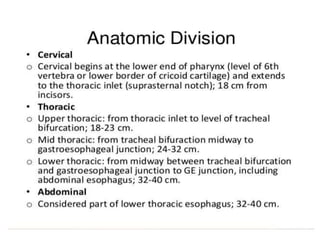
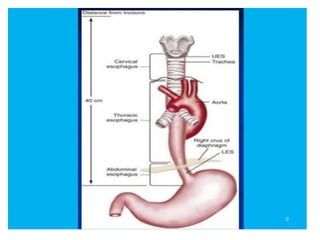
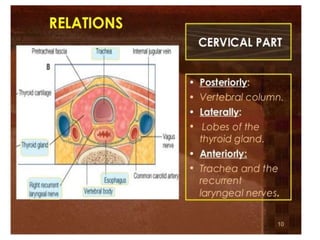
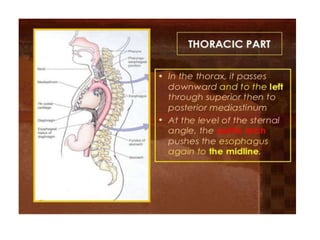
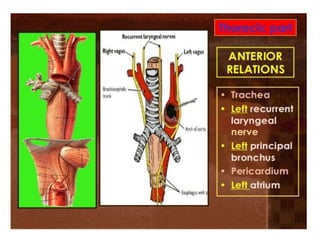
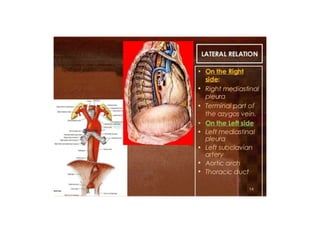
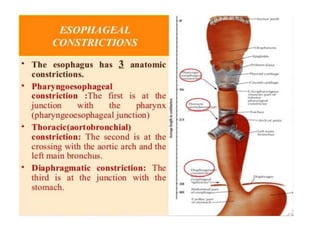
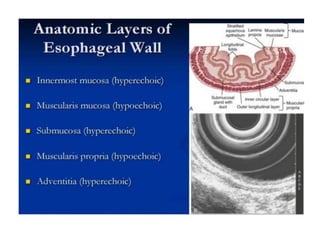
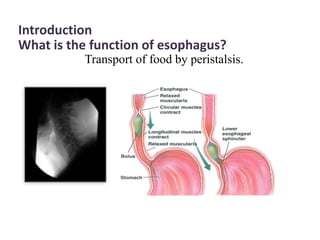
- Details of the anatomy of the esophagus and the indications for barium swallow studies such as dysphagia and heartburn.
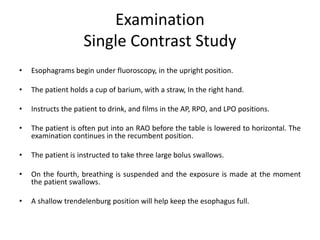
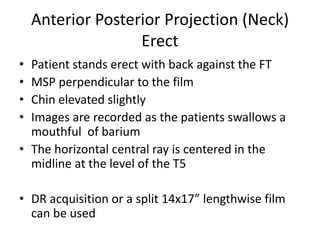
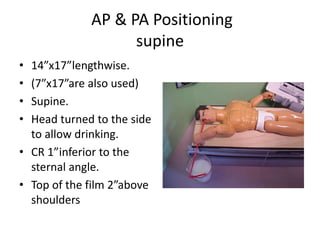
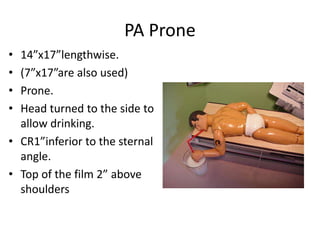
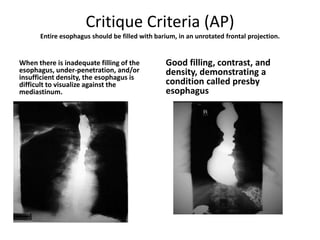
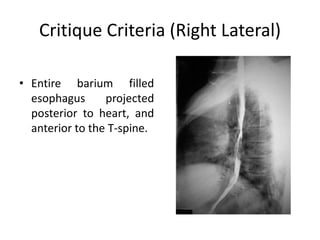
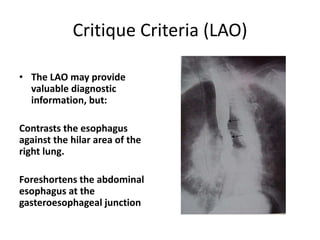
- The preparation, examination process, positioning, and critique criteria for barium swallow imaging including anterior-posterior, lateral, and oblique views.
- Additional imaging modalities that can be used such as CT and MRI are also mentioned.

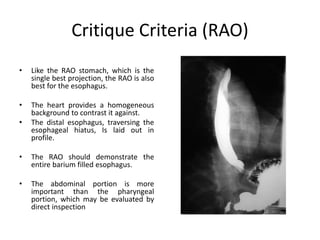



























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







